Project Completion
The patient and family engagement approach by Smith et al. (2017) was applied to a group of 30 people with diabetes. Upon their recruitment and the relevant ethical procedures, blood glucose was measured for them before the intervention; then, the intervention was carried out with the help of the Ottawa Model of Research Use (OMRU) (Graham & Logan, 2004; Logan & Graham, 1998). Eight weeks of the intervention were completed, after which the patients’ blood glucose was measured once again. The key findings are associated with the participants’ demographics and blood glucose.
Demographics
The demographics can be summarized as follows. All of the people recruited had diabetes. The slight majority of the participants were female (63%), 40-50 years old (60%) and with one comorbidity (specifically, hypertension – 50% or obesity – 10%). Additionally, 27% of the people involved had no reported comorbidities, and 13% had more than one additional condition. Figures 1-3 show the details of the demographics.
Blood glucose
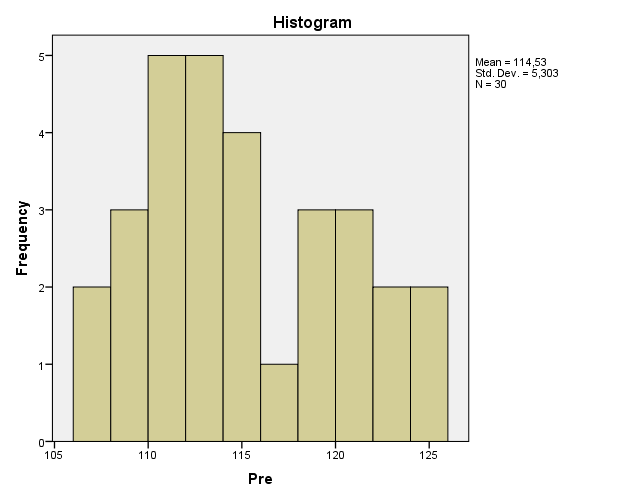
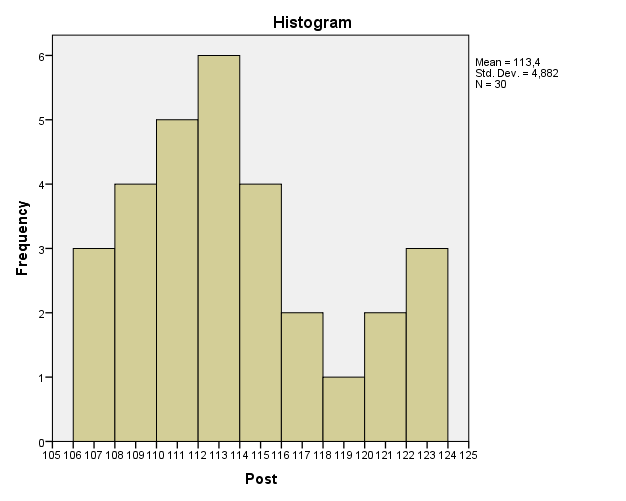
Blood glucose was measured, fasting, for the participants before and after education based on Smith et al. (2017). Additionally, blood glucose was monitored by the participants as a part of their diabetes management; no peaks were recorded over the course of the project. All the participants demonstrated blood glucose between 105 and 125 mg/dl. Sixty percent of the participants (18 people) demonstrated a reduction in blood glucose after the intervention. Figures 4 and 5 present the histograms of the pre- and post-intervention blood glucose in the participants.
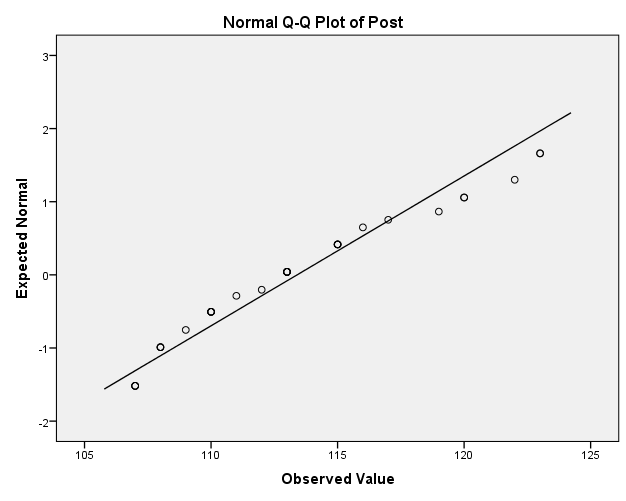
With the help of SPSS, the blood glucose data were explored and analyzed. First, the normality of the distribution of both datasets was checked with the help of the Kolmogorov-Smirnov and Shapiro-Wilk tests (see Table 1). Based on Shapiro-Wilk test, which is a more appropriate test for small sample sizes, the post-intervention dataset might be abnormally distributed. Looking at the scatterplot of the dataset (see Figure 6), this assumption appears reasonable. As a result, it is not helpful to use parametric tests for this project (Looney & Hagan, 2015; Polit & Beck, 2017).
Table 1. Tests of Normality.
It had been initially intended to use paired t-test for the task because of the specifics of the sample, which was supposed to be bigger, as well as the methodology (a pre- and post-test study). However, with the small sample, as well as the potentially abnormal distribution of the post-intervention data, it was more appropriate to use a non-parametric alternative. Polit and Beck (2017) recommend Wilcoxon signed ranks test as the suitable option since the project uses continuous data (see Table 2).
Table 2. Wilcoxon Signed Ranks Test.
As can be seen from Table 2, both the 2-tailed and 1-tailed tests return values that are greater than 0.05, which was the significance level set for the project. As a result, it is reasonable to state that the project cannot imply that the differences between the pre- and post-test datasets are statistically significant. Thus, the hypothesis about the effectiveness of the engagement method by Smith et al. (2017) in reducing blood glucose cannot be supported by the current project.
Discussion
Patient engagement in their care is a relatively new approach to healthcare (Bombard et al., 2018; Kim et al., 2018; Park & Giap, 2020). Diabetes, which is a very widespread condition with significant negative outcomes (National Center for Chronic Disease Prevention and Health Promotion, 2017; Zimmet, Alberti, Magliano, & Bennett, 2016), is among the conditions that require self-management, which makes various attempts to train and engage patients relevant for it (Quinn et al., 2018).
Furthermore, some evidence implies that the various methods of engagement, which include education and reconciliation, as well as consultations, may help to increase patient engagement levels, which are generally low, as well as possibly, with limited evidence, be associated with positive outcomes, including patient safety (Kim et al., 2018; Park & Giap, 2020).
These findings are applicable to diabetes as well; different interventions, including messages in a mobile-based patient engagement intervention (Quinn et al., 2018), helped to bring down blood glucose (Freeman, Hanlon, Denslow, & Hooper, 2018; Lee, Lee, Yoo, & Park, 2017). In the end, it is suggested that patient engagement is associated with blood glucose levels, and specific interventions were shown to result in improved engagement (Glenn, Nichols, Enriquez, & Jenkins, 2019). Thus, there exists some recent literature which implies that patient engagement measures might have an impact on blood glucose.
The findings of the present research cannot support the existing data about statistically significant improvements in blood glucose in patients. Here, it should be pointed out that the cited studies investigated the effects over prolonged periods of time (usually, half a year) while the current project only had several weeks (Freeman et al., 2018; Lee et al., 2017; Quinn et al., 2018).
Furthermore, the current project does suggest that over time, the blood glucose in the majority of engaged patients reduces; it is just that the results were not statistically significant, which may be attributable to the specific intervention used, the limited time of monitoring and, possibly, the small sample, which forced the project to employ a non-parametric test (Looney & Hagan, 2015; Polit & Beck, 2017). As a result, it should be highlighted that the research does not necessarily disprove the prior studies; rather, it cannot support them based on the currently available data.
The limitations of the project should be discussed in detail. First of all, the project is not a randomized controlled trial; it is a pre-test post-test study, which means that it does not guarantee the control of all extraneous variables (Polit & Beck, 2017). Furthermore, the sample of the project was relatively small, and the data distribution prevented the project from employing a parametric test, which are generally considered to be more accurate than non-parametric ones (Looney & Hagan, 2015; Polit & Beck, 2017).
Both these features mean that the findings might not be very generalizable. In line with that, it should also be mentioned that only the participants of one healthcare institution were involved; as a result, bringing the findings outside of those or very similar settings would not be appropriate.
As a result of these limitations, additional research may be recommended. It is noteworthy that the guide by Smith et al. (2017) has not been empirically studied before, which means that for the people who might consider implementing it, additional inquiry into its effectiveness might be helpful.
It is notable that the current research suggests a statistically insignificant drop in blood glucose of the participants; also, other research in the field implies that diabetic patient engagement is a promising endeavor which can improve blood glucose (Freeman et al., 2018; Lee et al., 2017; Quinn et al., 2018). Therefore, an additional test of the materials by Smith et al. (2017) that would involve a bigger (and, possibly, more diverse) sample over a longer period of time could produce more conclusive findings.
The value of the project can be described as follows. Aside from researching an intervention that was not studied before (that is, the specific Smith et al. (2017) intervention), it has a well-justified methodology that employs well-established methods, for example, the OMRU (Graham & Logan, 2004; Logan & Graham, 1998).
All the choices, including those that led to limitations, were explained by the needs of the project and feasibility considerations (especially as related to time and access to patients). It should also be pointed out that while nonparametric tests are not as accurate as parametric ones, they are extremely helpful for the cases of using abnormally distributed data (Polit & Beck, 2017).
Since the assumptions of the initially planned t-test could not be applied to the data, the decision to use a non-parametric test is very well-justified, and it can be claimed that the selected test is recommended by the relevant literature for similar cases (Looney & Hagan, 2015; Polit & Beck, 2017).
In summary, the presented research is not exactly in line with the existing literature since it does not demonstrate a statistically significant effect of the selected method by Smith et al. (2017). However, that could be explained by the project’s limitations, as well as the fact that the patient engagement approach by Smith et al. (2017) has not been studied before. The project contributes new evidence to the methods of engaging patients with diabetes in their own care, which is a very promising field. With a greater sample and longer timeframe, an additional inquiry into the topic could be very helpful.
References
Bombard, Y., Baker, R., Elaina, O., Bhatia, P., Casalino, S., Onate, K.,… Pomey, M. (2018). Engaging patients to improve quality of care: A systematic review. Implementation Science, 13(1), 1-22. Web.
Freeman, K., Hanlon, M., Denslow, S., & Hooper, V. (2018). Patient engagement in type 2 diabetes: a collaborative community health initiative. The Diabetes Educator, 44(4), 395-404. Web.
Glenn, L. E., Nichols, M., Enriquez, M., & Jenkins, C. (2020). Impact of a community‐based approach to patient engagement in rural, low‐income adults with type 2 diabetes. Public Health Nursing, 37(2), 178-187. Web.
Graham, I. D., & Logan, J. (2004). Translating research-innovations in knowledge transfer and continuity of care. Canadian Journal of Nursing Research Archive, 36(2), 89-103.
Kim, J. M., Suarez-Cuervo, C., Berger, Z., Lee, J., Gayleard, J., Rosenberg, C.,… Dy, S. (2018). Evaluation of patient and family engagement strategies to improve medication safety. The Patient – Patient-Centered Outcomes Research, 11(2), 193-206. Web.
Lee, M. K., Lee, K. H., Yoo, S. H., & Park, C. Y. (2017). Impact of initial active engagement in self-monitoring with a telemonitoring device on glycemic control among patients with type 2 diabetes. Scientific reports, 7(1), 1-7. Web.
Logan, J., & Graham, I. D. (1998). Toward a comprehensive interdisciplinary model of health care research use. Science Communication, 20(2), 227–246.
Looney, W. S., & Hagan, L. J. (2015). Analysis of biomarker data: A practical guide. Hoboken, NJ: John Wiley & Sons.
National Center for Chronic Disease Prevention and Health Promotion. (2017). National Diabetes Statistics Report, 2017. Web.
Park, M., & Giap, T. (2020). Patient and family engagement as a potential approach for improving patient safety: A systematic review. Journal of Advanced Nursing, 76(1), 62-80. Web.
Polit, D.F., & Beck, C.T. (2017). Nursing research: Generating and assessing evidence for nursing practice (10th ed.). Philadelphia, PA: Lippincott, Williams & Wilkins.
Quinn, C. C., Butler, E. C., Swasey, K. K., Shardell, M. D., Terrin, M. D., Barr, E. A., & Gruber-Baldini, A. L. (2018). Mobile diabetes intervention study of patient engagement and impact on blood glucose: mixed methods analysis. JMIR mHealth and uHealth, 6(2), e31. Web.
Smith, K., Baker, K., Wesley, D., Zipperer, L., Clark, M. D., Hanneke, C. R.,… Goeschel, C. A. (2017). Guide to improving patient safety in primary care settings by engaging patients and families. Web.
Zimmet, P., Alberti, K., Magliano, D., & Bennett, P. (2016). Diabetes mellitus statistics on prevalence and mortality: Facts and fallacies. Nature Reviews Endocrinology, 12(10), 616-622. Web.