Spencer County Community
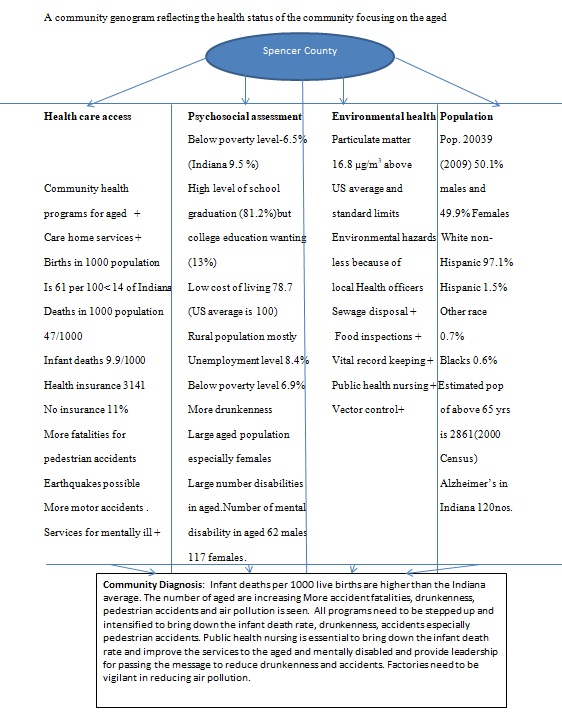
Spencer County had a completely rural population of 20,039 as estimated in 2009. Houses with occupants numbered 6316 while rented houses numbered 1253 (Spencer County, City-data.com). Renters formed 17 % of the population. The land area was 399 sq. mi. while the water area occupied 2.5 sq. mi. The population density was 50 people per square mile. An interesting finding was that the cost of living index in the county was much less than that of the US average; 78.7 to 100 in the US. Employment was offered by the manufacturing industry (28.2%), education, health and social services (15.6%), and retail trade (12.0%). Employees of the private institutions formed the largest group of 82%. Government employees made up 10% of the workers. Only 7% of the employees were self-employed. Whites formed the maximum number in the many races in Spencer County: 97.1% (Spencer County, City-data.com). The rests were Hispanics and blacks.
The median resident age was 37.3, lower than the Indiana age of 35.2. The males outnumbered the females: 10217 to 10174. Lesser people were below the poverty line in Spencer County; 6.9% when compared to the state level of 9.5%. The air pollution level was above the US average level at 16.8 µg/m3 and the standard limit at 15 µg/m3. The sulphur oxide level in the atmosphere was above the US average but below the standard limit (Spencer County, City-data.com). Foreign born residents constituted 16% of the naturalized citizens, much less than in the other parts of the state. Most of the population was married and most married couples were together. Widowed females were more than the males (Spencer County, City-data.com).
Agricultural resources dairy farming, crops like corn, wheat, soybeans and vegetables provided the income. Very few people with professional school degrees or doctorates were found in Spencer County though school enrolment was almost as good as Indiana’s.
Various statistics in Spencer County were below expected levels and the Indiana averages. Births numbered 1,257 in 2005 (Spencer County, City-data.com). The number of births was 11.8 in 1000 population in the county compared to 14 per 1000 in Indiana in 2004 and 2005. Deaths numbered 962 and the number per 1000 live birth was similar to the Indiana figure at 47. Till 2001, lesser infants were dying in the county. After that, the figure had been rising steadily in comparison to Indiana. This was probably because the rest of Indiana had improved its measures to contain infant deaths while Spencer County had not followed suit. The number of infant deaths per 1000 live births was 9.9 compared to the 8 of Indiana in 2006 (Spencer County, City-data.com).
Specific dangers affected this accident-prone county probably contributing to the higher death rate. Spencer County was known to have more vehicle accidents than Indiana. A similar picture was prevalent for drunkenness and fatal accidents. In 2006, suddenly there was a spurt of fatal accidents involving pedestrians: an average of 14.7 when compared to Indiana with 2 only while no such accidents were reported for the previous 3 years. Earthquake activity was higher in the county when compared to Indiana. The last was in 2008 showing 5.4 on the Richter. However, tornado activity was much less than in Indiana and the US (Spencer County, City-data.com).
Health concern
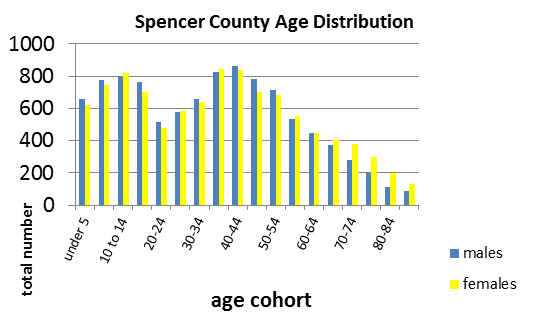
The condition of the aged was probably no better. We could infer that the females had the tendency to live longer. The sensory disabled, the physically disabled, the go-outside-home disabled, the self-care disabled and the mentally disabled all badly needed community health nursing (Spencer County, City-data.com). Focusing on the aged above 65 years, I have put together in a bar chart the statistics that were available for the disabled people above 65 years who came under the purview of the public health nurse in community nursing.
In the bar chart, I show the numbers of people above 65 years who have disabilities which they manage within their own homes or in group quarters. They do not have the facilities of institutions and they manage on their own or with the help of their family. Alzheimer’s patients are included in the mentally disabled group. This is the group that badly needs my help as a public health nurse. As 11% do not have insurance to help them through their difficult days, my help becomes necessary in empowering them in securing insurance for their needs in addition to assisting in their care. Blind people among the sensory disabled obtained the maximum supplementary security income in 2006 than aged recipients: 257against 75. This was unfair and here too my ability to empower the disabled aged for their rights must materialize.
The non-institutionalized mentally disabled would include patients with Alzheimer’s disease. The present health care facilities are not sufficient for the growing population of the aged. All disabilities are expected to increase in number and so these facilities would become insufficient (Spencer County, City-data.com). By the year 2000, 1840 households or 24% had one or more persons aged more than 65 years, 24 %. The institutionalized population was just 2000: this highlighted the situation of an inadequate number of institutions for people who were in need.
Population
Sixty two mentally disabled male patients and 117 similar female patients above 65 years needed the help of public health nurses. The population of the people above 65 years was estimated to be 2861 in 2006 (Spencer County Demographic Report on the elders, 2000). Population over 85 was estimated to be 339. Around 372 numbers would be present as estimated by the incidence of 13%. However, the actual number of patients found in Indiana in 2010 by the statistics of the Alzheimer’s Association was 120 which is far below the estimated level of 372 (2011). It is expected to rise in 2025 to 130. Spencer County would be having a share of the illness. This is my health concern. The rising incidence, the impossibility of cure and prevention, the increase in mortality due to the progress of treatment in other illnesses and the expected inadequacies of care by family members have motivated me for selecting Alzheimer’s Disease as my focus of concern.
Health equity and relevant data
Alzheimer’s Disease affects 5.4 million Americans (Alzheimer’s Association, 2011). This illness which was the sixth leading cause of death has now risen the scale. While other causes have reduced mortality, the deaths due to this illness have risen by 66%. The annual mortality rate due to Alzheimer’s was 26.2 as decided in 2007 (Alzheimer’s Association, 2011). This illness with dementia cannot be prevented or cured or slowed. The costs incurred in providing care for these patients have reached $183 billion (Alzheimer’s Association, 2011). Fifteen million caregivers are supporting the patients without getting any remuneration. The emotional and physical sufferings of the caregivers are significant with Alzheimer’s. Indiana has 320477 caregivers (Alzheimer’s Association, 2011). Depression has been reported in 33% of the caregivers. Thirteen percent of the aged above 65 are expected to have Alzheimer’s. Only 4 % have Alzheimer’s before 65 years. Two-thirds of Alzheimer’s patients are women. The people of Spencer County have a right to get the best of care and support for their Alzheimer’s patients. I am there for them.
Resources and partners
The public health nurse works in close collaboration with the health department and the local policymakers of Spencer County. The health department has a mission to work for the Spencer county community. Their job is to provide quality health services (Health Department, Spencer County). Their policies would promote healthy lifestyles. The disease would be prevented and protected against. The best public health would be maintained. My job is to hold hands with the health department and help to create a healthy environment and prevent disease and disability. It also requires me to empower caregivers in caring for the disabled including the dementia patients of Alzheimer’s.
Diagnosis
Age related changes and Alzheimer’s disease may be difficult to differentiate at the beginning of the latter illness. Ten signs have been used as the tools for the diagnosis of Alzheimer’s. Memory changes are expected in senility but if it causes problems in daily life, the option should be Alzheimer’s (Alzheimer’s Association, Seven counties). Executive functions like planning and solving problems are not possible anymore: these were done previously without any issue. Familiar tasks can no longer be done. There is confusion with time and place; the patients lose their way home due to this. Visual images are not understood anymore. The image of themselves in the mirror may be mistaken for another person and the patient may invite the other to come forward. The spatial relationships are similarly misunderstood. Speaking and writing become a chore. Forgetting how to do these is the problem. Misplacing things and forgetting how to retrace them is another issue. Patients have been known to keep hiding the same things repeatedly. The ability to judge is decreased or lost. The incapacities make them withdraw from social activities as they feel inadequate among people who knew them earlier. Mood changes are expected. Their personality becomes very different from their earlier ones (Alzheimer’s Association, Seven counties).
Outcomes or goals
Identification of the patients with this illness is the first action. The families must be ready to receive their ill member (Aging in place, Caring.com). The patient must be provided with a comfortable homestay without falling. She must be able to move around the house safely and with ease. The caregivers must be able to look after their patients without going into depression and all kinds of stress (Aging in place, Caring.com). Sufficient support will be provided by me for all these activities. The illness cannot be cured or prevented or delayed so interventions or preventive measures or delaying medicines do not have any effect. The compassionate care of the patient till death is the only goal behind my efforts.
Nursing actions
As a public health nurse, I aim to first identify the people with Alzheimer’s disease when suspicions are aroused. The warning signs mentioned above may be used. Families with new cases would be advised on how to receive the patient and how to “elder-proof” the house so that the stay is comfortable without avoidable accidents and hazards. The patient should live on the ground floor of the house. Grab bars and non-slip rugs are to be placed as necessary and in the bathrooms to prevent falls. Easily manageable door handles and kitchen gadgets may be placed. As the patient goes deeper into the illness, cooking may not be advisable as gas fuels may be left to leak with the potential to cause fires. Occasions would be plenty where family members need to be advised on the disabilities that go with the illness. The patients may have incontinence when catheterization becomes necessary. Advice will be given on keeping the catheters well and clean and ensuring that output is maintained. The families also need to know that the patient can be provided opportunities to utilize the brain through crossword puzzles, learning a new language and doing mathematical problems to keep stimulating his brain (Schwartz, Seven Counties). Daycare centres and other institutions have these opportunities. The families may be advised to take them to these places. Empowering the families to get insurance for these patients or security funds from the government would also be part of my nursing duty. The families and caregivers would need to put some time off for mending their stressful lives. They may have outings or picnics away from the patient while somebody else takes care.
Work to improve the health concern
The health activities that are propagated would change the norms practised in the community. The attitudes would be altered and awareness raised. The collaborative efforts with the community would create healthy environments which are disease-free and address disabilities that can be treated or prevented and those which cannot be treated or prevented like Alzheimer’s. An ecological approach may be necessary as a response to the needs of society. The ability to enhance development through the influence of policymakers is a duty of the public health nurse.
Partnerships
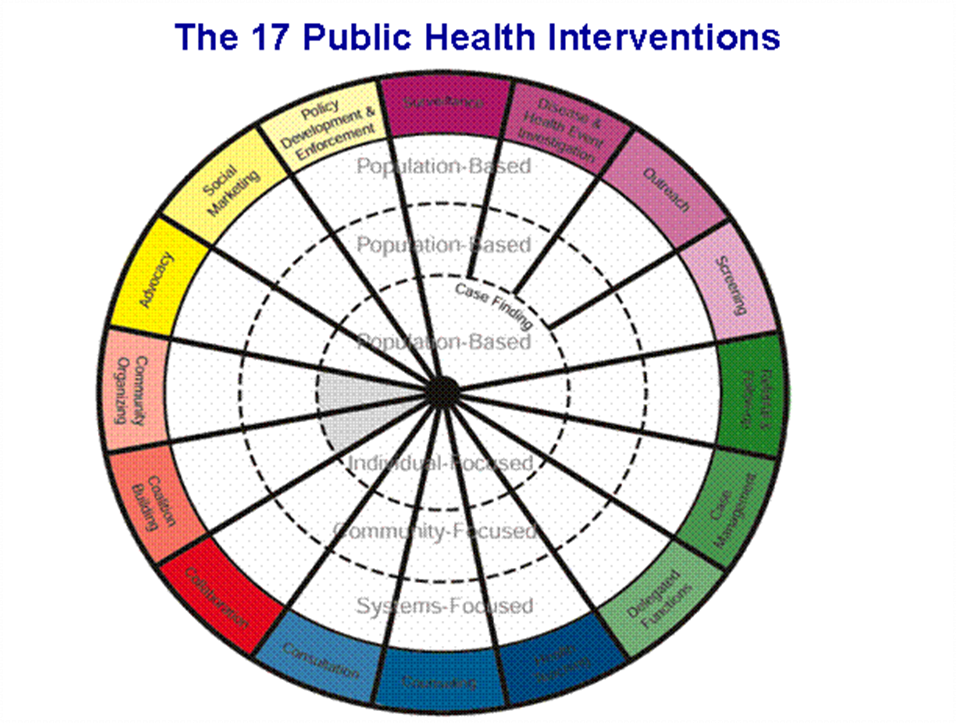
The multiple interventions that a public health nurse practices are indicated in the Minnesota wheel. She ties up with other health professionals to work with the community for common health gains. The duties that she has to undertake vary widely with the needs of the community she works in. Surveillance is one duty as a part of the multidisciplinary early intervention team which provides occupational and speech therapy and does social work. Compiling of reports would also be done by her. Occasionally she does outreach intervention for people in remote places. Case management and referral would be her duty. Performing delegated functions and health teaching are other responsibilities. In all the public health nurse collaborates with the leaders of the local community and other health professionals to meet the health requirements of the area. Counselling is a major function. This is what I would be doing for my health concern of Alzheimer’s disease. The intervention wheel on page 11 clearly defines the 17 interventions that a public health nurse is capable of. Partnerships would be with other health professionals, teachers, local leaders, religious heads and the families of Alzheimer’s.
Objectives for implementation
The objective for my health concern is to ensure that patients of this illness get all the care possible in the community. Their families must cooperate to ensure this good care. Care would be taken to provide adequate relaxation plans for the caregivers. Gathering community support for caring for these patients is essential. Educating the families and community on this non-preventable and non-curable illness is another objective. Arranging insurance and Government security income so that the patients are not found wanting in care due to poor finances is another objective.
Timeline
This program is not like that for any other illness where interventions would reduce the number as an outcome. Here the number being cared for well would be the outcome. No timeline is set.
Evaluation
It is difficult to determine this through statistics normally taken through Census estimations. However, the nurse and the community could do this evaluation by themselves for the record. The factors which govern good care and not-so-good care would be difficult to define. Indicators may have to be determined through collective discussion with partners.
Conclusion
My role as public health nurse would help me prepare society for caring for Alzheimer’s patients. Knowing for sure that my efforts are not going to reduce the number of Alzheimer’s patients or prevent or cure the illness, I believe it is my duty as a nurse to promote the best care for these doomed patients as long as they live. My help can also reduce the distress of the caregivers who are prone to problems of their own caused by their caregiving. Teaching them how to share the caregiving and arrange relaxation activities in between would improve their attitudes. Partnerships and collaborations with local community leaders would harness their support.
References
Aging in place.Web.
Alzheimer’s Association, 10 warning signs. Web.
Seven Counties Services Inc.
Alzheimer’s Association ( 2011) Alzheimer’s facts and figures. Web.
Health Department, Spencer county, Web.
Spencer County Demographic Report on the elders, 2000: An overview of Census 2000 Data. Web.
Spencer county, Indiana, Advameg Inc. Web.
Schwartz, A. Use it or lose it: the brain. Web.
Seven Counties Services Inc. Web.
The Intervention Wheel in Public Health Nursing, Wisconsin Dept. for Health Services. Web.