Literature Review
In the USA, chronic heart failure (CHF) is one of the most common causes of hospital readmission. Ziaeian and Fonarow (2016) report that medical therapies that are found to be beneficial for CHF outcomes and readmission rates are critically underutilized in patients. The authors highlight the following strategies for reducing the CHF readmission rate: extra support at discharge, ongoing communication, and early outpatient follow-up (Ziaeian & Fonarow, 2016).
A study by Feltner et al. (2014) has demonstrated that up to 25% of patients hospitalized with CHF are readmitted within thirty days. The systematic review has shown that current clinical practice for the care of adults with CHF after hospitalization is not standardized and, therefore, varies greatly (Feltner et al., 2014). The authors have identified the most effective preventive measures: namely, MDS-HF clinical interventions and home visitation programs are associated with a significant reduction in all-cause readmission and mortality.
Chronic heart failure hospital readmission is best tackled by STS that includes monitoring, health promotion, and self-care management using telephone technology. The nurses in the analyzed studies conducted a series of scheduled calls with specific objectives and structured interviews (Felther et al., 2014). Black et al. (2014) also describe a strategy that uses telephone monitoring and ongoing coaching between a patient and a nurse. The authors note that the described transition program needs to set off during hospital stay to allow for a smooth transition into everyday life.
Successful preventive strategies require the equal engagement of both a nurse and a patient. While health practitioners can do what is in their power when a person is hospitalized, after he or she is discharged, they need to be aware of self-management techniques relevant to their condition. A study by Sahebi, Mohammad-Aliha, Ansari-Ramandi, and Naderi (2015) has shown that the majority of the participants diagnosed with CHF (70%) did not apply preventive strategies properly. They scored very low on the test that was supposed to check their knowledge of self-care maintenance, self-care management, and self-care confidence (Sahebi et al., 2015).
As Sahebi et al. (2014) discovered, poor self-management in patients with CHF significantly correlated with the likelihood to be readmitted. Thus, one may conclude that enhancing knowledge among CHF patients would allow them to be more autonomous in handling their conditions. This specifically applies to these groups of people who are at a higher risk of CHF complications. Betihavas et al. (2015) proposed a nomogram that provides an absolute risk score for CHF readmission at 28 days and one year after discharge. The researchers argue that health practitioners need to pay more attention to elderly adults, those living alone, and individuals with comorbidities (Betihavas et al., 2015).
Methodology and Sampling
The present prospective study employs a randomized control trial design that aims at finding a correlation between nurses’ ongoing telephone support and interventions and lower readmission rates. The participants are recruited based on the following inclusion criteria: diagnosed with class I-III systolic or diastolic heart failure, living independently, and willing to participate in three-month research.
The respondents also need to be over 45 years old (since CHF is an age-related condition) and be able to speak, read, and write in English so that language barriers do not impede their interactions with health practitioners. The main exclusion criteria are major cerebrovascular diseases (such as stroke) and class IV heart failure. The sampling method is convenience sampling: the research team is to contact local hospitals to distribute information about the study and find those who might be interested. The research team strives for equal representation of men and women in the study and makes an effort to involve people with diverse ethnic and cultural backgrounds. All participants are to give written explicit consent before enrolling in the study.
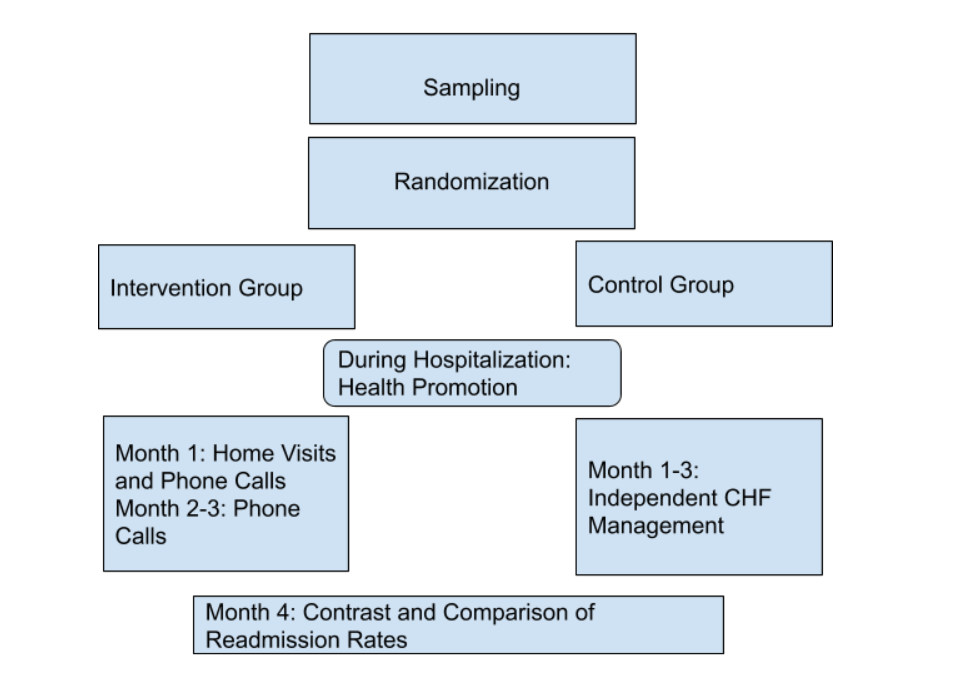
The participants are to be randomized and enrolled to control and intervention groups. All the participants have explained CHF management strategies during their hospital stay. Those in the intervention group are receiving home visits and scheduled phone calls within the first month after discharge, which is the critical period for those who have been hospitalized with CHF. After the first month, nurses only make phone calls, during which they continue coaching the participants on self-management and maintenance.
The patients in the control group do not receive any past support discharge; however, their status is closely monitored to track readmissions. It is expected that the participants in the intervention will be less likely to be rehospitalized as opposed to those who do not receive any home visits or phone counseling.
Successful realization of the study design will require handouts with key information on CHF self-management and devices for maintaining communication (telephones). Phone conversations need to be structured so that a nurse does not forgo a single step in patient assessment. To ensure a systematic approach to phone counseling, the researchers are to elaborate a script that a nurse could follow when making calls. The most important stages of the present research are depicted in the scheme below (Figure 1).
References
Betihavas, V., Frost, S. A., Newton, P. J., Macdonald, P., Stewart, S., Carrington, M. J.,… Davidson, P. M. (2015). An absolute risk prediction model to determine unplanned cardiovascular readmissions for adults with chronic heart failure. Heart, Lung and Circulation, 24(11), 1068-1073.
Black, J. T., Romano, P. S., Sadeghi, B., Auerbach, A. D., Ganiats, T. G., Greenfield, S.,… Ong, M. K. (2014). A remote monitoring and telephone nurse coaching intervention to reduce readmissions among patients with heart failure: study protocol for the Better Effectiveness After Transition-Heart Failure (BEAT-HF) randomized controlled trial. Trials, 15(1), 124.
Feltner, C., Jones, C. D., Cené, C. W., Zheng, Z. J., Sueta, C. A., Coker-Schwimmer, E. J.,… Jonas, D. E. (2014). Transitional care interventions to prevent readmissions for persons with heart failure: A systematic review and meta-analysis. Annals of Internal Medicine, 160(11), 774-784.
Sahebi, A., Mohammad-Aliha, J., Ansari-Ramandi, M., & Naderi, N. (2015). Investigation the relationship between self-care and readmission in patients with chronic heart failure. Research in Cardiovascular Medicine, 4(1), e25472.
Ziaeian, B., & Fonarow, G. C. (2016). The prevention of hospital readmissions in heart failure. Progress in Cardiovascular Diseases, 58(4), 379-385.