Introduction
Fetal Alcohol Syndrome (FAS) is a severe disease that has dangerous affects on the fetus and on a born child. Moreover, the abnormal features of this harmful syndrome accompany a person throughout the life span. The biological grounds of the disease are encompassed in the alcoholic effects going on in the body of the mother. It is no surprise that such an alcoholic reaction with harmful effects does not omit the fetus.
Postulated Mechanisms
Both direct and indirect mechanisms are discussed with respect to their contribution to alcohol-related effects on embryo-fetal growth and development. It is suggested that impairment in the protein synthetic machinery, resulting in cellular growth restriction at critical periods of development is the common mechanism underlying alcohol’s teratogenicity. Because the development of the CNS is so prolonged and complex compared to other organ systems, it is exquisitely vulnerable to derangement throughout pregnancy.
Transmission of impulses
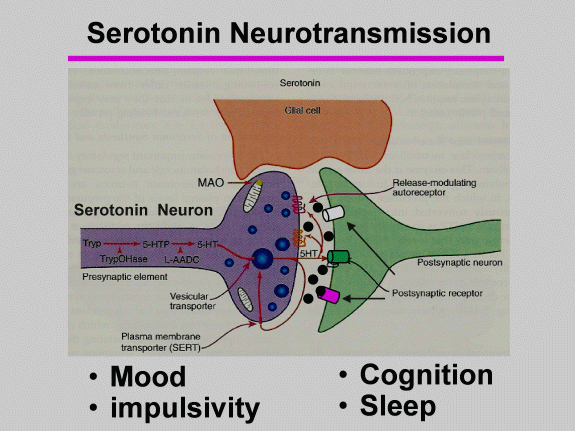
In the brain, there are a considerable number of Neurotransmitters. The significant Neurotransmitters related to alcohol are serotonin, glutamate and gamma-aminobutyric acid. Glutamate is the main excitatory Neurotransmitter.
Prenatal subjection to drinking can end up Triggering FAS, with symptoms of undeveloped limps, facial dysmorphologies, and much other neurobehavioral underdevelopment. Neurobehavioral impairments in Fetal Alcohol Syndrome, and in disorders brought about by drinking, encompass memory problems, concentration discrepancy, and motor dysfunction. A lot of the characteristics may be replicated in rodents.
The reported findings show that alcohol is the teratogen that commonly appeared among humans. However, scientists think that it can be solely prevented, for there is no cure to be used against the disease {235/2m}. This study is evaluated as a description and analysis of FAS’s harmful effect on both mother and child. Furthermore, the paper discloses the harms on different levels: biological, biochemical, physiological, social, and even economic. It means that the whole concept of the problem runs the gamut of the organism’s reaction to alcohol during pregnancy.
Thus, teratogenic impacts of alcohol are viewed as the key factors for the development of Fetal Alcohol Syndrome. Therefore based on available statistics, the research is implemented in terms of a deep estimation of FAS going on with supposed genetically related and physiologically impulse diseases and consequences on a child.
Methodology
Research and data of 81 mothers of young school-going children having PFAS or FAS are contrasted with142 haphazardly selected maternal controls of other children learning in the same schools.
The methodology used in this study is correlated in order to distill the main approaches and principles for working out the main problem. In this respect, a brief descriptive analysis of the disease itself is supported by peer-reviewed researches on FAS made in the US and overseas. Thus, generally accepted and unique features on the main issue are designated in terms of several questions that give a reason for FAS, namely:
- Why alcohol is so dangerous for infants and which trimester of pregnancy is the most hazardous?
- What are the factors maximizing the risk of FAS among pregnant women?
- Is there any amount of alcohol being of no harm to the fetus?
- What are the cure and stages of pregnancy on which it is better to use it?
- Are there any preventive therapies?
The variety of defects to a fetus is singled out so that to characterize the best method to be implemented in the study {514/3b}. The research is done in accordance with the current medical practice.
Case study
An examination of hazardous factors for extreme FSAD, FAS and other related disorders in an African society reportedly having a high number of these disorders globally was conducted.
Results and Discussion
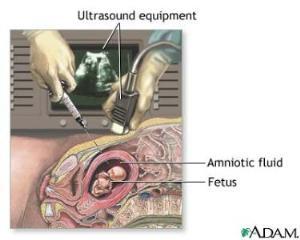
FAS is the result of the alcohol consumption of a would-be mother. This direct connection of a pregnant woman and a fetus inside is apparent. There is a scope of outcomes concerned with alcohol consumption: spontaneous abortion, growth retardation, facial abnormalities. A pregnant woman does not harm herself as worse, as she makes tragedy for a newborn child.
Fetal Alcohol Syndrome is considered with women who are alcoholics or those who drank too much previously. It is also a problem that can be inflicted during the first trimester of pregnancy when it is not well-known whether a woman is pregnant or not. The safe amount of alcohol to a fetus is not established yet {412/1t}.
Claire D. Coles provides points on FAS exposure delineated by attention deficit hyperactivity disorder (ADHD). Alcohol-related symptoms of FAS can rely on neurocognitive tests and clinical observation of children {199/2t}. This assumption shows that the roots of the disease are concerned with prenatal alcohol consumption. This is why the brain formation retards and perceives some physiological and genetic deformations, especially in the first trimester {545/3m}. Scholars (pediatricians, gynecologists, maieutologist, and therapists on the whole) should pay more attention to the special behavior of women to prevent FAS and its precursors as well.
Since FAS was first defined as a medical condition in 1973, sociologists relate it to the increase of sexual activity among adolescents and their illiteracy in the issue of normal sexual relations {7/5b}. Thus, the social-related implications are fully considered with the lack of educational and/or economic support. Further still, pregnant women exposing their children to FAS, place society at risk of adolescent delnquency12 {679/1t}. This application can be explained through the mental retardation which appears as a consequence of FAS. In turn, adolescents being invalid to think and act as fast as their peers seek appreciation by means of commission of a crime.
Therapists and pediatricians need time to work out if a child is healthy mentally and in terms of looks. Such observation of FAS was supposed in earlier studies to have similar effects as the syndrome of Down {239/2m}. However, children with attributes of FAS are not totally damaged in terms of mental activity. The main trouble occurs in their disability in thinking and speaking aspects. Their identification of the reality around them gets retarded. This detrimental factor begets a scope of supporting drawbacks that are inherent to a child throughout the life span.
One of the studies on FAS showed that the discrepancies that are distinctly obvious among infants in the age of 12 months than after 6 months by birth {617/4b}. These data help to estimate the preliminary treatment that can be done to a FAS-exposed child. It means that, in fact, the nature of the disease under analysis is neurodevelopment. Hence, it considers brain disorders and nervous system deviations on the whole.
The development of the fetus that is exposed to FAS can be aggravated by means of additional use of light and heavy drugs (cigarettes, marijuana, cocaine, etc. The abnormality of a child’s looks can get more ominous lines by birth. Since 2004 the major medical association and centers in the US agreed to include a new term concerned with FAS, namely: fetal alcohol spectrum disorder (FASD) {446/3m}. It concerns the use of alcohol itself and parallel substance abuse and other and other biologically-grounded factors within pregnancy.
There are various cases when pregnant women consume large amounts of alcohol and it does not affect a fetus. In this respect “playing with FAS” can play a box to a child. At least, it should not be something like drawing casting lots. The problem goes beyond one’s beliefs or expectations. It touches upon the medical implementation and the use of abstinence from alcohol during the period of pregnancy.
Qualitative interviews with a number of adolescents with alcohol-related mental disorders in the US high schools showed that the ability to commit a crime by an adolescent with FAS can be explained medically. In terms of anticipated trajectories implied, it became significant to state potential at-risk behaviors among children with FAS. In fact, socially, this disease provides an impulse for spontaneous or unpredicted negative deeds of a child that would be treated by him/her as normal. This evokes several assumptions on why there are so various and frequent cases of suicides among children and adults with FAS. It is known that adolescents with fetal alcohol spectrum disorders (FASD) in age from 5 to 29 are inclined to hurt themselves which was proved clinically {34/1t}. This is why therapists are suggested to provide communication with FASD individuals in terms of accurate choice of words and tone during the whole process.
There are different studies on preventive initiatives that are included in the program of many training centers for women exposed to FAS. In this respect to prevent harmful outcomes of FASDs experts recommend pregnant women make an intentional appointment with a set of doctors: pediatrician, psychologist, social worker, nurse, speech therapist, and physical or occupational therapist {365/3m}. Pre-natal therapies are concerned with being the most effective anti-FAS methods {160/4b}. Thus, FASDs can occur easily unless a woman decreases or stops drinking at all. This is outlined in terms of different studies. The reported ones state that the characteristics of children exposed prenatally to alcohol are quite consistent with how the full syndrome of FAS is defined today {103/2t}. Thus, a woman planning to have a child should think primordially of a healthy way of life during an ostensibly long period of time. Moreover, one can infer that a woman drinking too much prenatally cannot prevent a child from at least FASD when pregnant.
The probabilities of static encephalopathy and facial deformities along with severe neurobehavioral impairments cannot but omitted in both FAS and FASD students {6/5m}. The scope of such diseases can be expanded by retardation of recognition, slowness in realizing reality and reacting to different events. It gives a reason why everything related to the brain activity of an individual should not be impacted negatively from the inside, meaning alcohol consumption during the pregnancy.
Moreover, the quality of sperm during ejaculation of a constantly drinking father can influence harmfully on a child. The study reported by Viljoen et al. and concerned with the FAS problem in South Africa showed off that children with FAS had fathers who consumed 84.6 drinks per month, compared with 47.5 consumed by mothers both prenatally and during pregnancy {595/2t}.
Disinhibition theory alcohol is likely to increase the aggression among people who consume it and expose to it their generation {54/5b}. It means that the behavioral impairments can be easily inflicted chemically through alcohol in the blood of a mother to a child. Moreover, neuroanatomical studies claim that alcohol forces on the molecular structures within the brain and specific tissues during the gestational development of a fetus {174/1t}. It means that from the biochemical point of view alcohol is an aggressive component poisoning the nervous system and brain, particularly. In this case, one should take a look at the peculiarities of families in terms of different factors (stratification, economic, social, etc.). Here comes the question of whether alcoholism can be delivered genetically from parents to a child.
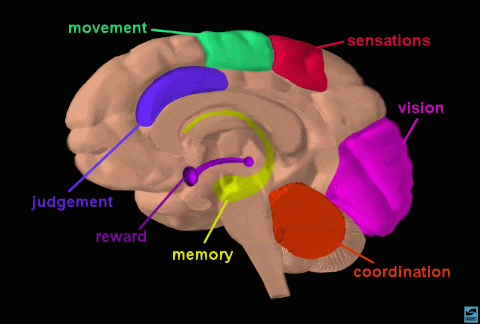
Continuing the problem of teratogenic influences of alcohol on the brain and behavior, it is important, to admit that despite total affection of the brain, the hippocampal area responsible for storing new memories becomes damaged seriously {187/2t}. Thus, the neurological and neurological characteristics of children and adults exposed to FAS or FASD need more attention on the part of therapists. It distills an idea following the prescription that neurons start decreasing or mutating if being affected by alcohol consumption intentionally (in the case with parents) and unintentionally (in the case with children).
When all data are gathered, it is about time to diagnose potential threats to a fetus and a child on the whole. Moreover, the studies reported by Earnest et al. indicate that alcohol impacts internal circadian clock function by means of loss of communication between neurons inflicted by the loss of cells {137/1t}. This becomes clear when talking about the loss of coordination among drunken people. It is obvious that the brain functions badly, thus its structure has got through partial destruction of cells.
Alcohol intake serves as a signal to the internal destruction of the whole nervous system. This is why to prevent women at risk of alcohol consumption from FAS and FASD, practitioners recommend counseling into gynecologic and obstetric care {219/1t}. It means that most of the controls can abstain from drinking if they are constantly motivated not to do it for the sake of the future child. However, testing cocaine-exposed infants in growth does not differ from alcohol-exposed children {44/4m}. This fact observed in the study outrages, as it becomes clear that there is no significant difference between consuming alcohol or heavy drugs. It influences the fetus similarly.
Exposure to FAS can affect the well-being of society. Thus, it is better to search for the reason among adolescent individuals, for risky sexual relationships often become a start for FAS. The studies reported by Miller et al. outline that 15% of FAS births among 4 million tested cases are to mothers under age 21 {521/1t}. Furthermore, $75 million and $9.7 billion per year are estimated to be the US government’s societal costs for solely 1% of live-born FAS infants {38/2t}. The low economic status of parents and a mother, particularly, has been suggested to be a reason for FAS emergence during pregnancy {773/5b}.
The implications on behavior peculiarities of children with FAS and FAE (fetal alcohol effects) are stated in terms of the Fetal Alcohol Behavior Scale (FABS) {55/3m}. To say more, the factors affecting children’s behavior are considered usually with a misunderstanding of their problems from outside (on the part of peers, adults, teachers, parents) as well as with inner pressure to react aggressively. According to Dunn’s conceptual model, there is a hypothesis that a continuum of interaction exists between neurological processing of sensory input and behavioral responses {265/2t}. This assumption was primordially proved in terms of the trickledown effect (abnormalities of the bones, heart, and genitourinary tract) caused by FAS {96/1t}. Such an evaluation of disorders happened to FAS and FASD-exposed children. Genomic, transcriptomic, and proteomic analyses in biology can help in identifying the essence and extent of alcoholic intoxication on a fetus {76/3m}. Hence, an observer should pay special attention to the neurobiological direction of alcohol intoxication as complemented the risk of FAS emergence.
Non-specific disruption of neuronal lipid bilayers caused by ethanol is apparent to the chemical explanation of the harmful effect of alcohol abuse per se {263/4m}. In its pure state ethanol is really dangerous for an organism. One of the problems that appear among FAS children, despite the aforementioned, is ocular disorders and affections of cataract{397/3m}. It provides a construct to hypothesize that the whole organism is exposed to disorders by means of alcohol consumption. Its severest form of negative influence can be achieved to a fragile forming of the fetus in which genetic and physiological information comes from the organism of a woman bearing it.
Comparing it to the above-stated information, it is no surprise that having ocular affection FAS-exposed children are hard to recognize visual information. In addition, children with FAS and ARND need more efficient interventions to reduce the extent or implementation of cognitive and behavioral impairments {155/3m}. All in all, the research on FAS and other alcohol-related disorders and diseases runs the gamut of reasons wherein consumption of alcohol is the main factor.
Due to respiratory activity assessed through cellular viability, it is known today that if a woman drank constantly prenatally it can fall into alcohol dependency during pregnancy {226/5m}. Thus, it is one more challenge to be faced by the medical communities and officials responsible for funding sources to reduce the problem of FAS. The dependence on alcohol is among the strongest like the dependence on smoking. Hence, would-be mothers or parents at large should keep a strict eye on their future today not to lag behind perspectives on health tomorrow. In the course of chemical analysis of the reaction that happened in the organism just after the alcohol consumption ethanol provides a range of metabolic reactions wherein acetaldehyde is a product of alcohol oxidation that is concerned with a bad smell in the mouth {246/1t}. Thus, the research somewhat comprehensively evaluates the dark sides of FAS imposed through alcohol consumption. Moreover, the empirical studies show that maternal attachment to a fetus is concerned with two main contributions: psychoanalytic (mother) and ecological (environment) {49/2t}.
Conclusion
In conclusion, FAS is supposed to be inflicted on a fetus through alcohol consumption of a mother during her pregnancy. In this respect, it does not matter whether it was during pregnancy or prenatally. All periods are considered to be at risk of FAS and FASD (along with ARND and ARDD) affection on a fetus and a child with long implications in the span of life. Pediatricians, gynecologists and, say, therapists should work out the methodology to treat and, perhaps, prevent the FAS and its symptoms prenatally and on the first through the third trimester of pregnancy. The fact that FAS is not cured at all does not mean hereby that no interventions should be applied to a mother and a child, particularly.
References
Wes.t, J. & Goodlett, C. Teratogenic effects of Alcohol on Brain Development. Pediatrics in Review. 22, 2001:47-55.
Clarren SK. Fetal Alcohol Syndrome. Disorders of development and learning. 2003: 235.
Fetal Alcohol Syndrome. Women’s Health Specialists. Web.
Campbell MK., & Farrell SO. Biochemistry. Ed. 6. Stamford, CT: Cengage Learning; 2007.
May PA., & Gossage JP. Estimating the Prevalence of Fetal Alcohol Syndrome a Summary. Alcohol Research & Health. 25, 2001: 159-168.
Cummings MR. Human heredity: principles & issues. Ed. 8. Stamford, CT: Cengage Learning; 2008.
Encyclopedia of Health. Vol. 7. Ed. 4. New York, NY: The Rosen Publishing Group; 2009.
Coles, CD. Fetal Alcohol Exposure and Attention: Moving beyond Adhd. Alcohol Research and Health, 25(3), 2001: 199-210.
Schonfeld AM., Mattson SN., & Riley EP. Moral Maturity and Delinquency after Prenatal Alcohol Exposure. Journal of Studies on Alcohol, 66(4), 2005: 545-555.
Boulter LT. The Effectiveness of Peer-Led FAS/FAE Prevention Presentations in Middle and High Schools. Journal of Alcohol & Drug Education, 51(3), 2007:7-12.
Lynch ME., Coles CD., Corley T., & Falek A. Examining Delinquency in Adolescents Differentially Prenatally Exposed to Alcohol: The Role of Proximal and Distal Risk Factors. Journal of Studies on Alcohol, 64(5), 2003: 678-679.
Schonfeld AM., Mattson SN., Lang AR., Delis DC., & Riley EP. Verbal and Nonverbal Fluency in Children with Heavy Prenatal Alcohol Exposure. Journal of Studies on Alcohol, 62(2), 2001: 239-247.
Coles CD., Kable JA., Drews-Botsch C., & Falek A. Early Identification of Risk for Effects of Prenatal Alcohol Exposure. Journal of Studies on Alcohol, 61(4), 2000: 607-620.
Magri R., Hutson J., Míguez H., Suarez H., Menendez A., Parodi V., et al. Advances in the Determination of Alcohol and Other Drug Consumption during Pregnancy: a Study of 900 Births in Montevideo, Uruguay. Contemporary Drug Problems, 34(3), 2007: 445-460.
Magnusson A., Goransson M., & Heilig M. Unexpectedly High Prevalence of Alcohol Use among Pregnant Swedish Women: Failed Detection by Antenatal Care and Simple Tools That Improve Detection. Journal of Studies on Alcohol, 66(2), 2005 157-165.
Hankin JR. Fas Prevention Strategies: Passive and Active Measures. Alcohol Health and Research World, 18(1), 1994: 62-70.
Ryan S., & Ferguson DL. The Person behind the Face of Fetal Alcohol Spectrum Disorder: Student Experiences and Family and Professionals’ Perspectives on Fasd. Rural Special Education Quarterly, 25(1), 2006: 32-43.
Huggins JE., Grant T., O’Malley K., & Streissguth AP. Suicide Attempts among Adults with Fetal Alcohol Spectrum Disorders: Clinical Considerations. Mental Health Aspects of Developmental Disabilities, 11(2), 2008: 33-41.
Educating Health Professionals about Fetal Alcohol Spectrum Disorders. American Journal of Health Education, 38(6), 2007: 364-372.
May PA., & Gossage JP. Estimating the Prevalence of Fetal Alcohol Syndrome a Summary. Alcohol Research & Health. 25, 2001: 159-168.
Green JH. Fetal Alcohol Spectrum Disorders: Understanding the Effects of Prenatal Alcohol Exposure and Supporting Students. Journal of School Health, 77(3), 2007: 103-115.
Ryan S., & Ferguson DL. On, Yet under, the Radar: Students with Fetal Alcohol Syndrome Disorder. Exceptional Children, 72(3), 2006: 363-371.
Viljoen D., Croxford J., Gossage JP., Kodituwakku PW., & May PA. Characteristics of Mothers of Children with Fetal Alcohol Syndrome in the Western Cape Province of South Africa: A Case-Control Study. Journal of Studies on Alcohol, 63(1), 2002: 6-17.
Kodituwakku PW., Adnams CM., Hay A., Kitching AE., Burger E., Kalberg WO., et al. Letter and Category Fluency in Children with Fetal Alcohol Syndrome from a Community in South Africa. Journal of Studies on Alcohol, 67(4), 2006: 502-523.
Viljoen DL., Gossage JP., Brooke L., Adnams CM., Jones KL., Robinson LK., et al. Fetal Alcohol Syndrome Epidemiology in a South African Community: A Second Study of a Very High Prevalence Area. Journal of Studies on Alcohol, 66(5), 2005: 593-602.
Gmel G., & Rehm J. Harmful Alcohol Use. Alcohol Research and Health, 27(1), 2003: 52-59.
Chen WA., Maier SE., Parnell SE., & West JR. Alcohol and the Developing Brain: Neuroanatomical Studies. Alcohol Research and Health, 27(2), 2003: 174-186.
Cicero, TJ. Effects of Paternal Exposure to Alcohol on Offspring Development. Alcohol Health and Research World, 18(1), 1994: 37-45.
Mattson SN., Schoenfeld AM., & Riley EP. Teratogenic Effects of Alcohol on Brain and Behavior. Alcohol Research and Health, 25(3), 2001: 185-194.
Bearer, CF. Markers to Detect Drinking during Pregnancy. Alcohol Research and Health, 25(3), 2001: 210-219.
Earnest DJ., Chen WA., & West JR. Developmental Alcohol and Circadian Clock Function. Alcohol Research and Health, 25(2), 2001: 136-145.
Maier SE., & West JE. Drinking Pattern and Alcohol-related Birth Defects. Alcohol Research and Health, 25(3), 2001: 168-176.
Handmaker NS., & Wilbourne P. Motivational Interventions in Prenatal Clinics. Alcohol Research and Health, 25(3), 2001: 219-227.
Day NL., & Richardson GA. Comparative Teratogenicity of Alcohol and Other Drugs. Alcohol Health and Research World, 18(1), 1994: 42-50.
Miller TR., Levy DT., Spicer RS., & Taylor DM. Societal Costs of Underage Drinking. Journal of Studies on Alcohol, 67(4), 2006: 519-526.
Bearer CF., Stoler JM., Cook JD., & Carpenter SJ. Biomarkers of Alcohol Use in Pregnancy. Alcohol Research & Health, 28(1), 2004: 38-53.
O’Connor MJ., & Whaley SE. Alcohol Use in Pregnant Low-Income Women. Journal of Studies on Alcohol, 64(6), 2003: 773-792.
Timler GR., & Olswang LB. Variable Structure/Variable Performance: Parent and Teacher Perspectives on a School-Age Child with FAS. Journal of Positive Behavior Interventions, 3(1), 2001: 48-52.
Franklin L., Deitz J., Jirikowic T., & Astley S. Children with Fetal Alcohol Spectrum Disorders: Problem Behaviors and Sensory Processing. The American Journal of Occupational Therapy, 62(3), 2008: 265-277.
Barrett JR. Trickledown Effect? Maternal Alcohol Consumption Linked to Cryptorchidism in Sons. Environmental Health Perspectives, 115(2), 2007: 96-101.
Gohlke JM., Hiller-Sturmhöfel S., & Faustman EM. A Systems-based Computational Model of Alcohol’s Toxic Effects on Brain Development. Alcohol Research and Health, 31(1), 2008: 76-85.
Davies M. The Role of GABA (A) Receptors in Mediating the Effects of Alcohol in the Central Nervous System. Journal of Psychiatry & Neuroscience: JPN, 28(4), 2003 263-272.
Hiratsuka Y., & Li G. Alcohol and Eye Diseases: A Review of Epidemiologic Studies. Journal of Studies on Alcohol, 62(3), 2001: 397-411.
Prenatal Exposure to Alcohol. Alcohol Research and Health, 24(1), 2000: 32-41.
Warren KR., & Foudin LL. Alcohol-related Birth Defects-the Past, Present and Future. Alcohol Research and Health, 25(3), 2001: 153-161.
Nagy J. Alcohol Dependence at the Cellular Level: Effects of Ethanol on Calcium Homeostasis of IM-9 Human Lymphoblast Cells. Journal of Studies on Alcohol, 61(2), 2000: 225-230.
Zakhari S. Overview: How Is Alcohol Metabolized by the Body?. Alcohol Research and Health, 29(4), 2006: 245-251.
Lewis MW. The Interactional Model of Maternal-fetal Attachment: an Empirical Analysis. Journal of Prenatal & Perinatal Psychology & Health, 23(1), 2008: 49-56. Web.