Introduction
Sepsis is a critical health condition in which the body reacts to an infection. Previous infections can sometimes pose serious risks to people because it leads to septic shock, where the body organs become overwhelmed, leading to organ failure (Lauriston et al., 2019). Sepsis is serious because it attacks critical body organs such as the lungs, gastrointestinal tract, urinary tract, and important body tissues. The disease is characterized by a sharp drop in blood pressure, multiple organ failure, high fever, and acute respiratory Distress syndrome-ARDS. All are happening simultaneously, which is why 40 percent of sepsis cases result in death (Centers for Disease Control and Prevention, 2022). It is vital to detect sepsis early to rescue a patient’s vital body organs from shutting down. If detected late, it is very difficult to reinstate the affected body organs to normalcy, making death imminent for such patients.
Brief Overview of Case Scenario
Pete Darby-not real name is a 40-year-old man living in Derby, Connecticut, and works as a construction site supervisor. Pete is married to Melinda, and they have three children together. Pete did not get sick often except for the occasional cold or headache. One Saturday afternoon, as he headed home from work, Pete felt a mild fever and brushed it off. On Monday, he reported to work, as usual; however, by 3 pm, Pete’s fever had worsened. Pete drove himself to a local health facility where the doctor prescribed Tamiflu for him and was sent home. On Wednesday, Pete could not report to work and complained of severe pain in his body, and his fever had gotten worse. His wife called an ambulance, and Pete was rushed to a nearby hospital. At the hospital, Pete’s body temperature read between 102 and 104 degrees and slight problems with breathing.
The doctors at the hospital tested for Sepsis and found that Pete’s body was already in septic shock. The local hospital could not handle this case as Pete needed a facility equipped with advanced treatment systems. Pete was rushed by an ambulance with the intensive care unit to the nearest facility equipped with advanced treatment equipment 260 miles away. At this time, Pete’s body temperature was extremely high, and his blood pressure had dropped down to dangerous levels. At the same time, Pete had developed acute ARDS, and his organs were shutting down. When he reached the hospital where he was transferred, Pete was diagnosed with a severe case of bacterial infection in his blood, and his body was reacting to the infection by shutting down his organs.
Significant Issues and why they occurred
Sepsis manifests rapidly, leading to multiple organ failures and death in a short time. As seen from Pete’s case, one of the significant issues in Sepsis is how fast a patient’s condition changes within a very short time (Lauritsen et al., 2020). For example, on Saturday, Pete felt a mild fever which he thought would go away in a few hours. By Wednesday, Pete was on ICU bed facing imminent death. This means that had Pete or his wife delayed seeking help on time, Pete’s organs would have shut down, and by the time they would rush him to a hospital, rescuing him would be a tall order. Another significant issue about Sepsis is that Sepsis has become one of the leading causes of death for Americans even though only a handful of people are aware of it.
Sepsis is a clinical emergency because millions of Americans die from the disease annually. More Americans are dying from Sepsis, making it a serious public health concern. Research by Sepsis Alliance shows that over 1.7 million Americans get Sepsis every year, out of which 270,000 people die from it (Sepsis Alliance, 2022). Further, Sepsis Alliance reveals that the number of deaths caused by Sepsis supersedes the number of deaths caused by AIDS, breast cancer, and prostate cancer combined annually. Besides, sepsis has become the leading cause of patient deaths in hospitals, especially in the ICU section. Based on these statistics, there is no doubt that Sepsis is a serious health condition that needs close attention.
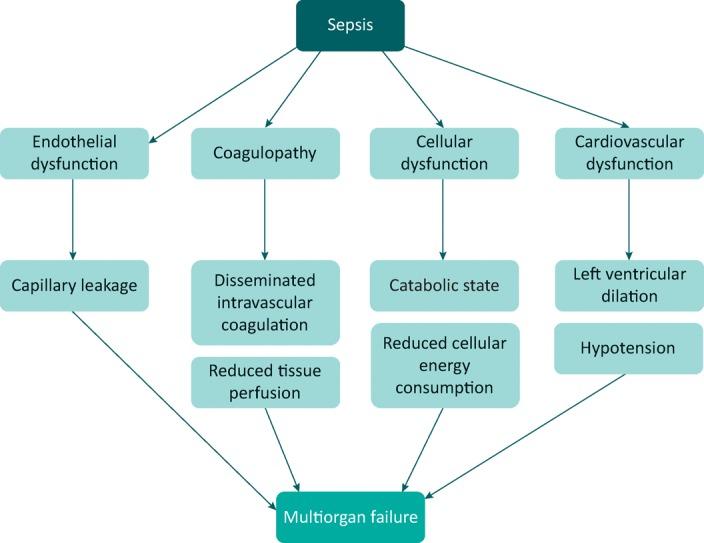
Sepsis is expensive to treat, which impacts patient outcomes. A majority of sepsis patients spend a considerable amount of their hospital stay in the ICU as they require close monitoring and advanced treatment (Somogyi and Sheridan, 2020). While it is difficult to determine the direct costs or expenses for extensive care, it is estimated that it consumes close to 30% of a hospital’s budget (Centers for Disease Control and Prevention, 2022). This means that a few individuals in intensive care are responsible for excessive resource consumption. As mentioned earlier, most sepsis patients end up in intensive care, which requires considerable financial resources on their part. The longer they stay in intensive care, the more expensive it becomes for patients and their families. Early detection of Sepsis helps millions of American families to save thousands of dollars that would otherwise go into the treatment of Sepsis in intensive care (Ng. Alexander and Frith, 2018). The diagram below shows the pathogenesis of Sepsis and how it manifests into a serious health emergency.
Relationship to Multidisciplinary Team
Dealing with sepsis requires high level of collaboration between health care inter-professionals such as nurses, physicians, and other primary care givers who directly deal with sepsis patients. Sepsis patients require round-the- clock monitoring since their condition deteriorate fast. Teamwork between health care givers has an impact on patients’ outcome. Through collaboration between Multidisciplinary Team, it is easier to detect errors done by others and correct them on time. Consequently, Multidisciplinary collaboration between health care professionals help to reduce sepsis mortality while improving patient outcomes.
How Sepsis Relate to my Patient on Treatment, Management and Nursing Care
Early treatment of Sepsis will definitely reduce the mortality rates. Being a medical emergency, Sepsis should be diagnosed early and, if detected, treated quickly. The first line of treatment for Sepsis is the administration of fluids and antibiotics as quickly as possible. Quick treatment of Sepsis is critical because with each passing hour without treatment, the risk of death for sepsis patients increases by an average of 7.6% (Villar, Short and Lighthall, 2019). Concerning antibiotics, a broad spectrum of drugs is used to deal with a bacterial infection. These antibiotics are administered intravenously so that they are quickly spread throughout the body efficiently and quickly (Mastrian and McGonigle, 2018, p.332). It is recommended that the intravenous antibiotics be started no later than one hour after Sepsis has been detected.
A combination of treatments is the most effective way of managing Sepsis. Unfortunately, antibiotics alone do not treat Sepsis. Doctors administer plenty of fluids to sepsis patients to stop the body’s blood pressure from getting dangerously low, leading to shock. Besides, adequate fluids help stop organ damage and help the organs remain stable and continue functioning normally (Mosier, Roberts and Englebright, 2019, p.545). The most common type of fluid administered to sepsis patients is the normal saline fluid, which contains critical minerals such as sodium. Within the first hour of treatment, oxygen must be administered to sepsis patients to maintain body oxygen level at 95% or higher (Mastrian and McGonigle, 2018, p.333). Other critical considerations in the treatment and management of Sepsis include the monitoring of patient’s urine every hour, close monitoring, assessing the condition of tissue hypoperfusion using non-invasive methods.
How my Clinical Example Supports my Arguments
The clinical example on Pete fosters the argument that many people are not aware of what Sepsis is. Like Pete, most people assume or brush away the symptoms of Sepsis because they do not know the disease. Most people react too late when a loved one’s organs have shut down to the point of no reverse. For example, Pete was lucky that his wife called an ambulance when he did. A few delays would have resulted in an undesired ending for the family. Secondly, the clinical example provided supports the argument that Sepsis leads to rapid deterioration of a patient’s conditioning, making survival chances very slim.
As documented in Pete’s case, what started as a mild case of fever on Saturday quickly progressed to a situation of intensive care by Wednesday. This factor goes to show how time is a critical factor when dealing with Sepsis. Everything from calling for help to first-line response has to be fast, right, and quickly to enhance a patient’s chances of survival. Quick action by doctors when a patient with Sepsis is brought to a hospital also helps to stop the rapid shutdown of critical body organs such as the kidney.
The provided case scenario augments my argument that regular monitoring of sepsis patients improved their outcomes. When patients with severe Sepsis are closely monitored, it is easier to detect deterioration and take immediate measures to correct the situation. For example, frequent monitoring of the patient’s tissue perfusion level and constant assessment of hemodynamic status helps to know the stability of a patient. Additionally, it is important for caregivers to continuously monitor a patient’s vital signs, urine output, blood pressure, respiratory rate, oxygen saturation, and heart rate (McGonigle, 2017). Performing these activities makes the difference between the survival and death of sepsis patients.
Implications for Future Practice
Early detection of Sepsis has implications for clinical practice guidelines. The Surviving Sepsis Campaign-SSC, the body charged with providing guidelines for dealing with Sepsis, asserts that early detection and quick/prompt treatment of Sepsis decreases mortality rate. The SSC statistics reveal that the mortality rate of septic shock is currently above 40%, making the disease one of the leading causes of death (Rhee and Klompas, 2020, p.589). Based on the knowledge that early detection of Sepsis reduces mortality rate. New evidence by health experts supports early detection and prompt treatment as the new guideline for reducing sepsis mortality rate and developed a new definition for the disease based on evidence (Goulden et al., 2019, p.350). For example, the Third International Consensus Definitions for Sepsis and Septic Shock-Sepsis 3 provides nurses and doctors with a detailed guideline for assessing and treating sepsis shock using the SOFA- Sequential Organ Failure Assessment score as well as qSOFA-quick SOFA. These new guidelines mean that doctors and nurses in the future must assess sepsis shock using SOFA and qSOFA guidelines.
How The Issue Relevant to Emergency Nursing Practice
The new definition of Sepsis will result in the capture of a broad spectrum and a large number of patients. The new definition of Sepsis has essentially lowered the lactate threshold for septic patients from a high of 4 mmol to a low of 2 mmol. The lowering of the lactate threshold is significant because it provides the ideal lactate value critical in predicting mortality in Sepsis (Morrill et al., 2019). This means that future practice for dealing with severe Sepsis and mortality in Sepsis must use the guidelines the updated guidelines on early interventions such as the use of antibiotics and intravenous fluids that remain the first line of responding to Sepsis.
Physicians based in low and middle countries face the challenge of adopting the Sepsis 3 definition and guidelines due to resources. In these situations, the doctors are forced to continue using the physical examination of Sepsis to know what type of pathogens are involved in causing Sepsis in their patients (Yan, Gustad and Nytro, 2022, p.560). Nevertheless, Sepsis 3 remains a new evidence-based approach of expediting the early detection of Sepsis and reducing the mortality rate caused by the disease.
Recommendations
Governments must educate their citizens to be more enlightened and aware of Sepsis. Most sepsis deaths occur because millions of people do not know what it is, so they respond rapidly if they suspect the disease. For example, many people only call for help/ambulance when the critical body organs have begun shutting down due to septic shock. If people have more awareness about the disease, they will go for checkups and treatment at the earliest opportunity, which is critical in reducing mortality (Jabour et al., 2021, p.2963). Sepsis is a life-threatening situation that calls for quick action from both the patients and doctors/nurses.
Caregivers/physicians must adopt the new Sepsis-3 guidelines for early detection and management of Sepsis. The new Sepsis-3 approach provides a new definition of Sepsis that is critical for early detection of sepsis and quick response to the (Dameff, Clay and Longhurst, 2019). The approach provides a protocolized treatment for patients with Severe Sepsis. The advantage of the protocolized treatment approach of Sepsis is that it reduces incidences of multi-organ failure and dysfunction, leads to improved outcomes, and reduces sepsis mortality rate (Singer, 2019). It is also recommended for doctors to adopt the Sepsis-3 protocols of assessing Sepsis because it provides an expanded view of Sepsis (Howitt et.al. 2019, p.510). Previously, Sepsis was simply defined and identified as an inflammatory response to an infection.
Conclusion
Sepsis is a life-threatening situation that calls for rapid response and treatment. Many sepsis patients do not make it out alive because they took too long to call for help. Time is a critical element in dealing with Sepsis because every passing hour without treatment increases mortality risks. Thus, Sepsis is a clinical emergency because millions of people die from the disease because they do not know what it is. Secondly, early detection of Sepsis is critical because it reduces organ failure/dysfunction. Organ failure is what leads to the death of sepsis patients because organs shut down when they cannot contain the pain and pressure of septic shock. Early detection helps doctors restore the organs to normalcy, stabilizing the body. New approaches and guidelines such as Septic-3 are critical for the early detection and management of Sepsis. Septic-3 impacts future practice because it provides a protocolized treatment of Sepsis, leading to better outcomes
References
Centers for Disease Control and Prevention. 2022. Sepsis is a life-threatening medical emergency. Centers for Disease Control and Prevention. Web.
Goulden, et al. 2018. QSOFA, SIRS and NEWS for predicting in hospital mortality and ICU admission in emergency admissions treated as Sepsis. Emergency Medicine Journal, 35(6), pp.345-349.
Somogyi, R. and C. Sheridan, D. 2021. Recent Advances in Bedside Device-Based Early Detection of Sepsis. Journal of Intensive Care Medicine, p.08850666211044124.
Dameff, C., Clay, B. and Longhurst, C.A., 2019. Personal health records: More promising in the smartphone era? Jama, 321(4), pp.339-340.
Howitt, et al., 2018. Incidence and outcomes of Sepsis after cardiac surgery as defined by the Sepsis-3 guidelines. British journal of anaesthesia, 120(3), pp.509-516.
Jabour, et al., 2021. The Patient Reported Outcomes as a Clinical Tool (PROACT) Pilot Study: What Can be Gained by Sharing Computerized Patient-Reported Mental Health and Substance Use Symptoms with Providers in HIV Care? AIDS and Behavior, 25(9), pp.2963-2972.
Lauritsen, et al., 2020. Early detection of Sepsis utilizing deep learning on electronic health record event sequences. Artificial Intelligence in Medicine, 104, p.101820.
Mastrian, K. and McGonigle, D., (2018). Cognitive informatics: An essential component of nursing technology design. Nursing outlook, 56(6), pp.332-333.
Mosier, S., Roberts, W.D. and Englebright, J., 2019. A systems-level method for developing nursing informatics solutions: The role of executive leadership. JONA: The Journal of Nursing Administration, 49(11), pp.543-548.
Morrill, et al., 2019. The signature-based model for early detection of Sepsis from electronic health records in the intensive care unit. In 2019 Computing in Cardiology (CinC) (pp. Page-1). IEEE.
Ng, Y.C., Alexander, S. and Frith, K.H., 2018. Integration of mobile health applications in health information technology initiatives: Expanding opportunities for nurse participation in population health. CIN: Computers, Informatics, Nursing, 36(5), pp.209-213.
Rhee, C. and Klompas, M., 2020. Sepsis trends: Increasing incidence and decreasing mortality, or changing denominator? Journal of Thoracic Disease, 12(Suppl 1), p.589.
Sepsis Alliance. 2022. What Is Sepsis. Sepsis Alliance. Web.
Villar, J., Short, J. H., & Lighthall, G. 2019. Lactate predicts both short-and long-term mortality in patients with and without Sepsis. Infectious Diseases: Research and Treatment, 12, 1178633719862776.
Yan, M.Y., Gustad, L.T. and Nytrø, Ø., 2022. Sepsis prediction, early detection, and identification using clinical text for machine learning: A systematic review. Journal of the American Medical Informatics Association, 29(3), pp.559-575.