Introduction
Congestive heart failure, which is often abbreviated as CHF, is a condition that one’s heart is not able to pump sufficient blood to the other parts of the body (Kinchin 204). The condition can happen in a gradual process or a in a rapid process. The CHF conditions can be aggravated by a wide range of related conditions like high blood pressure, the coronary heart diseases and other diseases that are related to the heart (Kinchin 204).
Previous studies (Heerdink 995; Burke 206) have indicated that approximately two million people living in the United States alone become victims of the congestive heart failure (CHF), while an average of 500 000 admissions of new cases are witnessed every year. In previous studies conducted in Italy, a statistics of 200 000 patients were suspected or confirmed to be victims of CHF in the cardiology units. In all those reported cases, 40% of the entire patient’s population was reported to be in need of admissions in the hospitals (Heerdink 95). There are various new therapeutic measures that have been laid down, in an attempt to bring down the statistics of the CHF cases. Despite all these efforts, a very recent study indicated that the occurrence of the CHF cases has not changed much. This study can be backed up by the observable diminishing fatality chances from the status of acute cardiovascular occurrences that later result in a large statistics of those who are at risk of being infected with CHF. In the contrary, it is indicated that regardless of the condition remaining in a stable condition, the occurrence of the CHF condition is stipulated to be on the rise. This is as a result of aging in the general population and the related consequence that that comes along with the condition in the health care facilities which is probably increasing (Heerdink 188; Burke 206).
Cardiovascular heart failure has been considered a very lethal and fatal syndrome, with its rates of mortality being referred to that of the fatal forms of cancerous cases. The CHF condition has been considered a very dangerous condition with its occurrence to be constantly in the increase, in the contrary it is worth wondering why the cases of the condition that receive admissions in the hospitals has been on the increase over the years. The increase has been revealed on very steady escalating rates that produce a very steep graph. In the United States, CHF is now considered the most renowned cause of hospital admissions, with majority of the patients being 67 years and above (Porche 56; Demetrius 200).
Problem Statement
CHF is an issue affecting many people and public health systems in different countries across the world. More than 20 million people worldwide are affected by CHF while 2% of prevalent patients are reported in developed countries. Nasi and Alahmad (2004) note that the American Heart Association has reported that there are 5.3 million Americans suffering from the CHF condition with 660,000 new patients being reported annually. The occurrence of the condition is about 10 people per 1000 persons in the U.S. population. Due to health implications brought about by the CHF condition, about 287,000 people die every year. In spite of increased infection rates of CHF, the success rate of treating the conditions has also increased (Georgiou, et al. 2001). On the contrary, the problem remains high in rural settings that are characterized by high readmissions of CHF patients. Therefore, this study investigates reasons for high CHF patient readmission in a local setting (Jong, et al., 2002).
Hypothesis Statement
The research will satisfy the following questions.
- Does the month of January register the highest number of CHF admission and readmission?
- Is non compliance the major reason for CHF readmission?
- Can a case management strategy be used to mitigate the rising number of cases of admission and readmission of CHF patients?
Rationale and significance
Cardiovascular heart failure has always caused a major strain on many health care facilities such as in the cardiology units and the general departments related to medicines, which takes initiatives in caring for CHF patients (Porche 56; Demetrius 200). Most importantly, intervention measures should be identified to ensure improvements of the prognosis and in the implementation of strategies that are aimed at reducing the cost incurred in the treatments (Porche 56; Demetrius 200). Consequently, it is worth identifying the factors that act as the predictors of a long time hospitalization and which may result in hospital mortality.
Summary
There are a number of factors that are attributed to CHF conditions. These risk factors which expose individuals to the risk of contracting the CHF condition include alcohol intake, smoking, lack of PCP follow up, non compliance to medication and lack of community follow ups. In addition, other medical conditions that can increase the risk of CHF conditions includes overweight or obese, diabetes, hyperthyroidism and other heart related diseases (Heerdink 195; Burke 206). This paper aims at identifying the relationships between such risk factors and the patients who are hospitalized with CHF condition.
Literature review
Cardiovascular cases have been associated with a variety of factors such as age and sex. The age and sex factors have been considered a health risk to the condition (Marantz 175; Tobin 65; Derby 199). Despite cardiovascular diseases being the greatest health challenges in the current centaury, the condition is found to be popular among those aged 65 years and above (Porche 48, Demetrius 202). It is reported by (WHO 205) that over 1.6 million cases were observed globally. The cardiovascular conditions have always been used to investigate and evaluate the potential impacts and effects of the secondary diagnosis and other related contributing factors. Several studies have also revealed that more men are prone to the condition compared to females. Relevant surveys have also indicated a positive relationship between low to moderate physical activities because men are more statistically observed to suffer from contributing medical conditions such as diabetes, or high blood pressure. Other factor that can contribute to the CHF condition is lifestyles of people. CHF condition is significantly observed in the elderly because they are less physically active in comparison with active children and youths (Porche 17; Demetrius 200). It has been observed that successful maintenance of health to avoid CHF condition is to lose excessive weight through involving in regular and vigorous activities. Sporting have always been associated with a positive impact in promoting of health-there is a positive effect on the CHF factors in the maintenance of a good health through sporting activities (Porche 134; Demetrius 44).
CHF conditions are the fifth ranked leading global cause of death. A report by WHO (201) indicated a high rate of global morbidity and mortality in over 2.8 million people of adults. CHF conditions have been reported to accounts for 44% of global diabetes mortality, 23% of global ischemic heart related diseases mortality and an average of 7% and 41% of high blood pressure conditions mortality. All these related diseases are casual etiologies that enhance mortality rates with the association of CHF conditions (Dryden-Edwards 210; Marantz 234; Tobin 78; Derby 94).
United States has been identified as a CHF condition holoendemic country, with obesity as the primary manifestation of the situation as the contributing factors (McMurray 200). The country is large enough with many mainlands as its components. The country has a large population, of which around 200 million people is the population of the Caucasian community in the country (Heerdink 87; Marantz 67; Tobin 45). The large immigrants who come from different countries from all over the world have attributed the very diverse cultures experienced in the country. Only 2.4% of the population in United States is the indigenous people population.
The economy of a country can be associated with that of Western-style capitalist, which can be attributed to the Western influence in the country with the immigrants from the Western worlds. Modernizations in most countries seem to follow the Western cultures, and this could be a major factor as well. According to the recent studies, the country has diverted an average of $8500 million on the health and care of CHF conditions treatments and medications. In the United States society, overweight is as a common phenomenon. More men than women have been surfer from overweight, with a 48% and 30% respectively from the population. In addition, the number of women who suffer from obesity exceeds the number of men who suffer from the CHF, with an observed average of 19% and 22% respectively from the population. The study also noted and documented CHF conditions in both the children and adults as victims of CHF conditions. United States is no exception in the global trend towards the increased cases of CHF conditions as seen in other many countries (Heerdink 199; Marantz 45; Tobin 94). The trend can be associated with change of the way of life and customs and modernization as a major factor contributing to the conditions.
The observed increase in the trend can be attributed to the kind of lifestyle that is associated with the people in the environment. This lifestyle can be described as a sedentary life, where many people do not involve themselves in physical activities. This lifestyle exposes the patients to a lifestyle with very many predisposing factors. This kind of life is common in both developed and developing countries (Heerdink 95; Marantz 67; Tobin 199). Making changes in the dietary methods can help in lowering the CHF risk factors. It is indicated that high consumption of sodium components can help in the maintenance of the body liquids, and as a result, the heart becomes overworked, which eases breathing.
It is thus advisable to take a limited amount of sodium on daily basis. These factors are associated with the increase in CHF conditions in the United States and the rest of the world (McMurray 213). The change of dietary in the society is a force to reckon with, as it has been observed as the major cause of body CHF conditions. The intake of junk foods is also associated with overweight and obesity, which is a major risk factors in the CHF conditions. The intake of junk foods has been on the increase in the developed and developing countries (Marantz 234; Tobin 94).
CHF has been associated with various diseases which are related to cardiovascular diseases, which has a very high mortality rate in many parts of the world. The cardiovascular diseases alone claim an average of 50,000 lives annually (Heerdink 195; Marantz 78; Tobin 14). Cardiovascular diseases are very common with the diabetic cases, which also affects various aspects of life, such as reducing the sufferers’ life expectancy by about 15 years (Porche 52). CHF conditions have been observed to be related to a number of complications such as many muscular-skeletal diseases, which leads to muscles wastage, and joints degenerations.CHF conditions complications involve cancerous conditions, in addition to psychosocial problems. Reports have shown that approximately 1.7 billion adults were CHF victims and at least 400 million people were diagnosed (WHO 200). The prevalence of the cases of the CHF conditions has continued to be on the rise regardless of medical measures that have been laid down to control the situation. Apparently, weight loss and weight maintenance as well as observance of a healthy diet is an ideal intervention for this particular condition.
Substance use and smoking is also a major factor in the CHF conditions. Studies have revealed that smocking damages the blood vessels. This causes a reduction in the amount of oxygen that is in circulation in the blood, a condition that results burdening of the heart (McMurray 28). The ultimate solution to this would be stoppage of smoking habits. Excess consumption of alcohol can also lead to weakening of the heart muscles. Weakened heart muscles are often characterized with abnormal heart rhythms. Individuals should avoid the excess consumption of alcohol in order to maintain healthy heart coordination (Dryden-Edwards 201; Marantz 65; Derby199).
Some information of great significance and relevance to statistics by Premier Beattie indicated that the total population of the world consists of specific groups. For every three patients, two are males. Half of the total population of female is CHF positive. Surprisingly, one out of every four of the children in United States is overweight (McMurray 213), and one out of three overweight people are literally obese cases. This evidence shows that a very large population is subjected to the cardiovascular diseases.
Cardiovascular diseases is a highly characterized complication of obesity disorder, with approximately 7000 people in United States dying annually of cardiovascular mediated diseases. In addition, an average of 20 people dies every day in relation to weight problems. From the observed statistics in studies, it is worth concluding that there is a crisis. This crisis is constantly on the rise with the cardiovascular diseases problems in the country. In the contrary, according to the Premier, about 1% annually, there is a 50% increase in the rates of CHF conditions and obesity cases in a period of 2 decades, which can be translated to a 5% annual increase of CHF conditions (Dryden-Edwards 201; Marantz 45; Tobin 266; and Derby 199). General, CHF condition is a troubling issue that affects many societies, particularly because its remedy is not forthcoming. Score of nations’ population have succumbed to CHF conditions as a result of poor eating habits. In addition, lack of adequate physical exercises has contributed to the escalation of CHF conditions (Dryden-Edwards 200; Marantz 143; Tobin 64; Derby 1594).
Studies conducted in the University of Queensland indicated that one out of every five adults in Queensland is obese or suffering from CHF condition (McMurray 188). Elsewhere, a survey by the Healthy Kids Queensland and Physical Activity was carried out for Queensland health strategies and nutrition tendencies. The study investigated the effects of physical fitness and weight management among children as well as between the ages of 50 years and above. The studies indicated that out of the total adults, 21% of them are struggling with CHF conditions. 19.5% of this population facing CHF conditions was males, while 22.7% were females. This statistics shows that obese and CHF conditions among males and females continue to be on the increase in Queensland. The population in Queensland has been observed to engage in a sedentary lifestyle. Actual values indicate that one male out six males are following the national guidelines of one of the moderate unhealthy dietary on daily basis. This trend has been observed in one out of every five female. In addition, one out of every four children in Queensland is found to be suffering from CHF conditions (McMurray 63).
High blood pressure is another factor that contributes significantly to the CHF conditions. Those who experience poor blood pressure are at experiences high risk of CHF conditions (Porche 14; Demetrius 24). Those who have poorly maintained blood pressure stand at a high risk of getting CHF conditions compared to those with normal blood pressure (Smith 26). High blood pressure causes the heart to be engaged in excessive work; hence straining the heart muscles. In order to put up with the increased work load, the heart muscles can increase in their width measurement and eventually lead to weakening of the heart muscles while gradually dilating (Demetrius, 20). The increased heart pressure and the changes that take place in the whole system may finally lead to heart failure.
Martensson et al. (25) maintained that patients with CHF may suffer depression as a result of frequent readmission, environmental changes, and increased financial demands. Consequently, the patients may hesitate from seeking timely medical checkup which worsens the condition. The perception that that the patient holds to the particular illness is therefore worth understanding, as it may influence the choice of intervention. This means that home care can as well be preferable as compared to hospital care, if at all it can cut on costs. Martensson et al. (56) found home care of CHF patients coupled with nursing follow up, to be a very effective way of managing this condition. This is particularly because the patients felt more secure and emotionally stable while living closer to their families. Consequently, the patients are likely to recover fast and hence reducing readmission rate. Furthermore, support and motivation from family members and friends while at him keeps them free from depression and mental disillusionment.
Methodology
Introduction
The research technique that shall be used is quantitative technique, whereby the data collected shall be graphically analyzed to draw some conclusion. The participants will be those the patients diagnosed with CHF condition, but must fall under the targeted age group. Economic and social status shall not count in the identification of sample group. Lawrence Hospital which has a bed capacity of 300 has been identified as the study environment. The study will basically rely on medical records alone, for data collection.
Research Design
The research will use quantitative descriptive design by doing retrospective chart review of cases diagnosed with congestive heart failure admitted in the local hospital. The data will be gathered between dates of January 2010 up to March 2011 period. Regardless of sex, number of admissions, ages sixty five years and above, either from other facility or from home admits. Also highlighted in this research are the indicators of re admission such as diet, medication, smoking, drinking, sedentary lifestyle, or no support from the community program.
The number of admission data will be presented as linear graph. The reasons for admission will be gathered and graphed for presentation. The study will start by obtaining permission to access the medical records department for chart review study on CHF cases admissions. Once obtained, charts will be gathered and screened with the inclusion criteria such as patients must be 65 years old and above, diagnosed with CHF, admitted during the study period of January 2010 to March 2011. Obtaining data by doing chart review will exhaust an estimated time of 4 days, 4 hours a day that will be split to 2 hrs in the morning and 2 hours in the afternoon. This will cover the 15 months of CHF admission charts. Tabulating and putting into graphs will take 3 days to finalize the input and findings. Due to time constraints, this chart review was opted to speed up the study process and meeting the deadline. The admission case will be graphed in linear form that will highlight the highest and lowest month/year of the admission. The reasons for admission will be in linear graph as well, that will be presented and followed by discussion of findings.
Setting
The study will be conducted in Lawrence Hospital, a community hospital with 300 bed capacity, in the suburb of Bronxville, New York. The target audience in this study was patients that were diagnosed with CHF when admitted or readmitted in the hospital from January 2010 to March 2011. Participants were 65 years old and above, regardless of sex, gender, marital status, socio economic status, and race. The population of elderly will be considered either admitted from home or any nursing skilled facilities, and rehabilitation center. Regardless of mental capacity or physical disability as long as patient admitted with CHF and falls on age category will be sampled. The patients’ ethnicity and cultural background will not be a problem in this study since this is only a chart review. Patients coming from different area in the local community will be sampled as well.
Study Participants
The community hospital has record of all the patients being admitted and coded the diagnosis. The study will be conducted in the local community hospital. The sampling technique will be used is the non probability purposive sampling. Target population of the study will be patients admitted with CHF ages 65 years old and above, regardless of sex, gender, race, and economic status. The main source of information will be the medical records of the patient in the hospital. The constraints of the study might be the process in obtaining access to the patient’s medical records. The study will gather cases of congestive heart failure admitted from January 2010 to March 2011. Reviewing charts with readmission of CHF cases between the months of January 2010 and March 2011.
Data Collection
Data to be collected
The data will be gathered are as follows;
- Diagnosis of CHF
- Patient 65 years old and above
- Reasons for admissions that includes non compliance to medications, no diet modification, alcohol intake, smoking, no follow up to PCP (primary care provider), lack of community support
- Admitted between dates of January 2010 and March 2011
The four data mentioned above plays the major part of the study. This research will not use questionnaire, interview, tests, survey, or actual patient interaction. This research will only use the medical records of the patients’ admission data and course in the hospital.
Procedure
The research will use quantitative descriptive design by doing retrospective chart review of cases diagnosed with congestive heart failure admitted in the local hospital. The data will be gathered between dates of January 2010 up to March 2011 period. Regardless of sex, number of admissions, ages sixty five years and above, either from other facility or from home admits. Also highlighted in this research are the indicators of re admission such as diet, medication, smoking, drinking, sedentary lifestyle, or no support from the community program. The number of admission data will be presented as linear graph. The reasons for admission will be gathered and graphed for presentation.
The study will start by obtaining permission to access the medical records department for chart review study on CHF cases admissions. Once obtained, charts will be gathered and screened with the inclusion criteria such as patients must be 65 years old and above, diagnosed with CHF, admitted during the study period of January 2010 to March 2011. Obtaining data by doing chart review will exhaust an estimated time of 4 days, 4 hours a day that will be split to 2 hrs in the morning and 2 hours in the afternoon. This will cover the 15 months of CHF admission charts. Tabulating and putting into graphs will take 3 days to finalize the input and findings. Due to time constraints this chart review was opted to speed up the study process and meeting the deadline.The admission case will be graphed in linear form that will highlight the highest and lowest month/year of the admission. The reasons for admission will be in linear graph, which will be presented and used for discussion and findings.
Survey Tool
The data collection tool used in this study was a research designed spread sheet. A spreadsheet is designed with 2 columns to include months/year and the number of admission. The second spread sheet includes the indicators for admission and comprises seven columns that includes the following date( month/year) and reasons for admission (non compliance to medication, no follow up to primary care provider, drinking alcohol, smoking, and lack/no support from community). Data from the study were collected from the chart where patient been admitted and discharged. Permission for access to the records was granted by the Medical Records Department head and the Hospital Director.
Interpretation of Analysis Result
The findings of the study indicate that the level of CHF patients in the rural setting fluctuated over the period from January 2010 to March 2011. The patients were as high as 17 in January 2010 (Piepoli et al., 2004). They declined to a low level of 5 patients during the month of May 2010 before beginning to increase gradually to 16 patients during the month of March 2011 as indicated in the figure below.
The increase in the level of CHF readmissions was attributed to be various factors such as non-compliance to medication, smoking, drinking alcohol and lack of diet modification as illustrated and explained below.
Summary
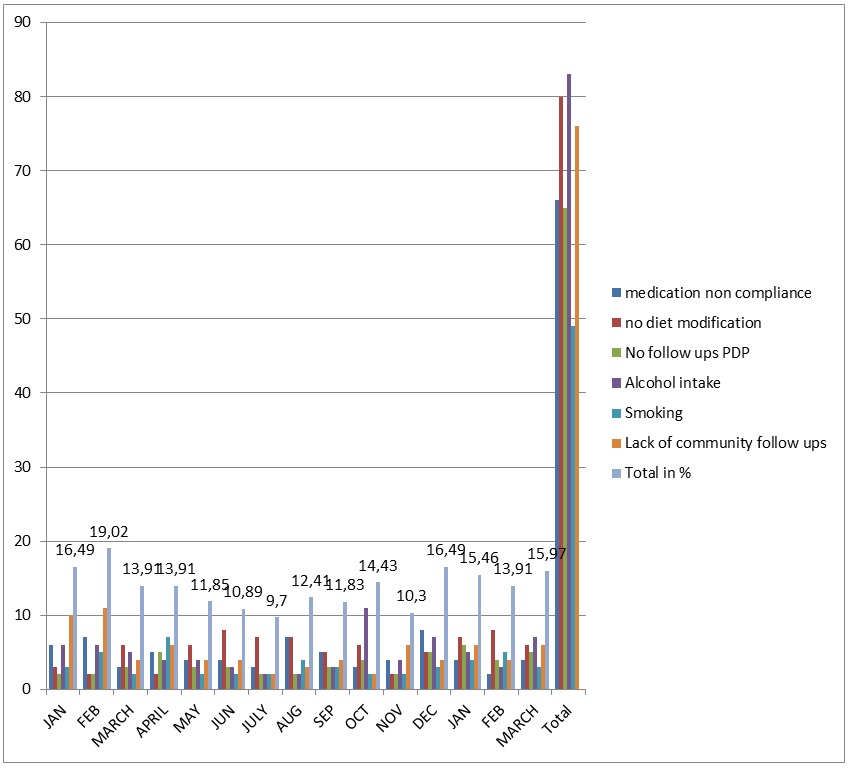
Figure I shows total number of patients who were admitted in the hospital on monthly basis for the whole 15-month period. Figure II illustrates the prevalence of medication non-compliance, no diet modification, no follow-ups PCP alcohol intake smocking lack of community follow-ups. The second table showed the patients. According to figure II, most admissions of patients were victims of CHF conditions whose cases were aggravated by the excessive intake of alcohol. Some 83 patients throughout the population study represented this. This was the highest number confirmed so far in relation to the CHF risk factors. The second popular risk factor among the patients was the non-modifications of diets, which was represented by 80 patients out of the possible 194 patients who took part in the study.
The third largest risk factor was due to lack of community follow up activities by the community. This was probably due to negligence by the community to carry out follow up activities on those who were already previously suffering from CHF condition. This was followed by a non-compliance of medication, which contributed, to a population of 66. Lack of follow-ups for PCP came to the second last risk factors according to the risk factors that were of study, with a population of 65. Lastly, the contributing factor that was recorded with the least number of patients was smocking. From the results, it can be deduced as to which factors puts one at more risk than the other.
Results Findings
Overview
According to the study, the predisposing factor or the risk factors have different pathogenicity while some factors are found to be more common among the patients than the other factors. From the study, it is noted that those patients who got involved in alcohol intake were the majority of the patients in the hospital at all seasons of the study. Alcohol intake has always been associated with the damaging of the heart by infecting the heart cells. Due to damages on the heart cells, the heart fails to contract sufficiently due to the weakening of the heart muscles, as a result, the CHF condition develops. This condition can be termed cardiomyopathy (Porche 12; Demetrius 222). Lack of diet modification was also featured as a leading factor. Consumption of food with high contents of cholesterol congests in the arteries that supply the heart with blood. This accumulation narrows the blood. As a result, this causes a reduction in supply of oxygen in the heart, which can result to cardiac arrest. In the extremes, heart failure occurs.
. The community non follow-ups and non-medical compliance were significant factors in the study- which contributed greatly to the aggravation of the CHF condition. Failure to comply with medical requirements impacts negatively on health status of patients. When the ventricles are damaged and fail to receive sufficient medication, they fail to function properly. This condition is known as systolic failure (McMurray 203). These conditions need to be diagnosed as they have different treatment mechanisms. These are some of the conditions that can result from failure to comply with medical requirements.
Analysis of the Data
Does the month of January register the highest number of CHF admission and readmission?
Although the month of January is not characteristically the only one that registers very high number of CHF condition, it is clear that substantial numbers of admissions are experienced at this particular month. Indeed, the highest value at 18 was recorded in the first January while the subsequent January still recorded relatively high level at 12. The trend also shows that the numbers of admission drops drastically after January, and also increases after December. From the analysis, it has been established that lifestyles and behaviors of individuals; such as alcohol intake are some of the leading CHF risk factors. Perhaps, it can go without saying that alcohol indulgencies and related behaviors during the month of December, which is a festive season has significantly contributed to the high number of admissions in January.
Is non compliance the major reason for CHF readmission?
None compliance to medical instructions is not the major reason for CHF readmission. It comes after no community follow ups, alcohol consumption and lack of dietary modification. Even though, an important risk factor that cannot be overlooked, some other risk factors seems to take a center stage. This shows that most patients are keen to comply with medication requirements, but some other factors such as alcohol intake results to readmission.
Can a case management strategy be used to mitigate the rising number of cases of admission and readmission of CHF patients?
Apparently, the study shows that there are some common patterns behind CHF admission and readmission. For instance, there is very high level of admission on January, and alcohol intake has been found to be a major risk factor. This case can be used as a strategy to mitigate the escalating number of CHF admission and readmission.
Result and Interpretation
Several risk factors of CHF have been identified, but some seems to have more impact than others. Alcohol has been found to be the leading risk factor leading to CHF condition. In addition, some periods such as January have registered very high level of CHF admission and readmission, something that can be attributed to behavioral indulgencies such as alcohol intake during the festive season of December.
Summary
In summary, the risk of CHF is basically contributed by behavioral factors, which can be adjusted if proper care is given to the patients. Nurses should follow up on CHF patients to ensure that they do not expose themselves in activities such as smoking, alcoholism, poor dieting habits among many others. They should also ensure that they adequately follow medical godliness to avoid readmission on similar cases.
Discussion and Conclusion
Overview
CHF is a frequent in hospital admissions and can be fatal if adequate care is not taken. A variety of risk factors have been found to contribute to the conditions. Managing CHF requires a coordinated and a well thought strategy in order to avoid hospital readmission. To achieve this, different factors that lead to hospital admissions and readmission should be studied and analyzed so as to take collective measures. This study has revealed that factors such as alcoholism are leading risk factors that increases CHF hospital admission and readmission. The study has also led to the realization that some months have more CHF prevalence than others; something that reflects back to seasonal behaviors of individuals, which predisposes them to CHF condition.
Discussion
Research Question1
The month of January is one of the leading seasons with high rate of CHF admission and readmission. This can be attributable to factors such as alcohol intake during the festive season of December. This is especially because alcoholism is one of the leading CHF risk factors as the study reveals. To reduce CHF hospital admission and readmission, individuals should be encouraged to live better lifestyles without engaging in excessive alcohol among other retrogressive behaviors.
Research Question2
Although non compliance to medical guidelines is not a major factor for CHF hospital admission and readmission, its occurrence cannot be overlooked as it contributes to some risky exposure. Patients should be encouraged to follow medical instructions to the letter.
Research Question3
Apparently, assessment of a particular case can successively be sued to mitigate the number of patients admitted and readmitted with CHF. This is especially because the risk factors that increase hospitalization of CHF can be identified and appropriate intervention undertaken.
Implication
This study has come up with findings that can have important implications to nursing and healthcare. The several factors that have been identifying as CHF risk factors can be used by nurses to device appropriate intervention for clients with CHF. Most importantly, nurses can give behaviors such as alcoholism a priority while intervening in CHF cases.
Limitation
Although the knowledge gained in this study is meant to be generalized in a similar situation, collection of data from a single hospital proves to be a big limitation. In addition, the sample size chosen in this study is relatively small, and mar not act as a good representative of a wider population.
Recommendation
This study recommends that health professionals should consider several factors that lead into proliferation of CHF in our society. Specifically, the professionals take careful consideration main risk factors such as alcoholism while designing a CHF intervention. All in all, CHF patients should be encouraged to avoid risk factors that can lead them to hospital readmissions.
Conclusion
Many factors have been founds to increase the chances of getting GHF. These factors include alcoholism, failure to follow medication guidelines, smoking, and lack of follow ups. Although all these factors are critical and are worth consideration while designing a Medicare intervention, some factors such as alcoholism which carries more weight than others need a closer attention. This notwithstanding, the impact of perception of patients to Medicare should be considered. For instance, some patients are likely to register low hospital readmission when attended from their homes particularly because they feel emotionally stable because of the support they receive from the family members and friends. Overall, a broad analysis of factors leading to CHF hospital admission and readmission is important if an effective intervention is to be come up with.
Works cited
Auble Hsieh ,McCausland, Yealy DM. Comparison of four clinical prediction rules for estimating risk in heart failure. Annals of emergency medicine 127–35.2005.56, Web.
Berger, Frank. Dissociative fugue stress disorder: PTSD. 2006. Web.
Berthold, Tim and Miller, Jennifer. Foundations for Community Health Workers. New York: John Wiley and Sons, 2009. Print. Web.
Burke, Edmund. Healthcare: Political representation. Stanford University. 2006. Web.
Carlson Lee , , Goroll Leahy, Johnson Ralph. “An analysis of physicians’ reasons for prescribing long-term digitalis therapy in outpatients”. Journal of chronic diseases 38 (9): 733–9, 1985. Web.
Cline, Israelsson, Willenheimer Broms., Erhardt Lambat. Cost effective management program for heart failure reduces hospitalization. Heart, 80, pp. 442-446. 1998. Print. Web.
Farhann Hossain., and Archi Tse N. “House democrats who voted against the health care bill.” New York Times. 2009. Web.
Felker Thompson, Hare Male. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. N Engl J Med. 2000. Web.
Heerdink Erk. Clustering of drug use in the elderly Population based studies into prevalence and outcome. Utrecht, The Netherlands 1995. Print. Web.
John Porche , Demetrius Angello. Public and community health nursing practice, a population-based approach. New York: SAGE, 2004. Print. Web.
Konstam, Dracup , Baker. Heart failure: evaluation and care of patients with left ventricular systolic dysfunction. Clinical practice guideline No. 11. AHCPR publication No. 94-0612. Rockville MD: Agency for Health Care Policy and Research; 1994. Web.
Kinchin, Dily. DID: The Invisible Injury. Oxford shire: Success Unlimited. 2004. Print. Web.
Krumholz Chen, Wang Vaccarino, Radford Horwitz. “Predictors of readmission among elderly survivors of admission with heart failure”. Am. Heart J. (1 Pt 1): (2000). Web.
Marantz Pattho, Tobin Joss., Derby Cohan, and Cohen Douglas. Age-associated changes in diastolic filling: Doppler E/A ratio are not associated with congestive heart failure in the elderly. South Medical Journal, Vol. 87, pp. 728-735. 1994. Print. Web.
McMurray Donagh, Morrison Corrie, Dargie Hill.Trends in hospitalization for heart failure in Scotland. European Heart Journal. 1993. Print. Web.
Meyers William P. America: Healthcare: Republic or Democracy? Stanford University Press. 2006. Web.
Ogden Bazzano, LA, et al. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study. Arch Intern Med. 2001. Web.
Pfeffer Miller, Braunwald Edmond, and Moye, Lee. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med Vol. 327, pp. 669-677. Web.
Schiraldi, Daniel, epersonalization disorder: A Guide to Healing, Recovery and Growth. New York, NY: McGraw-Hill, 2009. Print.
Smith Willson. Epidemiology of congestive heart failure. American Journal of Cardiology, Vol. 55, No. 3. 1985. Print.