Abstract
Accurate documentation of vital signs and CTAS scores is crucial to guarantee that patients are well treated. The provided research delves into the problem to assess the knowledge of the procedure among nurses and its impact on outcomes. Forty nurses took part in the research by answering the questionnaire.
The data shows that the enhanced knowledge of CTAS reduces resubmission rates and significantly improves the quality of treatment. The research compares data among hospitalized and emergency room patients and nurses’ knowledge of the intervention and evaluates outcomes. In conclusion, CTAS and its knowledge are essential for modern healthcare and should be included in nurses’ work.
Introduction
In the fast-paced environment of the Emergency Department, accurate documentation of vital signs and CTAS scores is important to ensure patients receive appropriate and timely care. The aim of this experiment was to assess the knowledge and comprehension of these critical documentation procedures among 40 ED nurses. The unit provides services to patients in usual and emergency room settings. More than 100 health workers provide services to patients with diverse needs that require care. The aim was to screen and document all patients within the time frames indicated, emphasizing collecting vital signs within 15 minutes of arrival and repeating vital signs within 60 minutes.
This study aims to assess 40 Emergency Department (ED) nurses’ expertise in reporting vital signs and the Canadian Triage and Acuity Scale (CTAS) score for all ED patients. The questionnaire’s unanimity highlights the relevance of CTAS encoding in ensuring that all patients are checked before admission to the ED. The recommendations underline the need for departments to evaluate and improve their systems to ensure timely and accurate documentation.
Literature Review
The Emergency Department is the first line of defense in healthcare, handling anything from minor injuries to life-threatening infections. The existing body of literature states that accurate recording, particularly of vital signs, is a critical component in ensuring that appropriate treatment is provided as quickly as feasible. Failures in such documentation, according to the research, might result in misdiagnoses, delayed treatment, and, in some cases, adverse patient outcomes. Moreover, Cotton et al. highlighted the value of CTAS encoding, which aids in patient prioritizing based on illness severity.
In such a way, the literature on the topic evidences the critical importance of CTAS and the need for its use in various settings, including emergency rooms and departments. Most authors acknowledge its positive impact on outcomes, patient satisfaction levels, and reduced readmission rates. Unfortunately, while many healthcare professionals recognize the need for this documentation, there is still a gap in its regular use, frequently linked to issues such as excessive patient influx, understaffing, or a lack of proper training.
Methodology and Data Collection
A detailed questionnaire was presented to 40 ED nurses to assess their comprehension and use of vital sign recording and CTAS grading. The rationale for using this measure is its ability to collect qualitative and quantitative data about the issue under research. Additionally, the validity and reliability of the tool are ensured by including relevant questions about the problem, effective sampling techniques, and the collection of credible data among professionals who work with clients.
The data was collected by distributing the questionnaire online or during the personal meetings. Everyone agreed that CTAS encoding and vital sign reporting based on baseline values were essential. The frequency and timeliness of recording varied, with some nurses reporting difficulty documenting within the time constraints specified owing to high patient numbers or concurrent emergencies. Thus, the baseline measurement showed that around 30 nurses avoided using CTAS or forgot about it.
The intervention was created as an educational and training module, emphasizing the importance of timely documentation and its impact on patient care. Senior ED nurses, a healthcare quality analyst, and a hospital IT department representative comprised the project team (to address any technical issues with the documentation system). Change resistance, technological problems, and the need for ongoing reinforcement training were all predicted hurdles. To ensure sustainability, the training was included in the onboarding process for new nurses, and periodic refresher courses were planned. Thus, it was assumed that the intervention would work for several reasons.
First, CTAS and measuring vitals are essential for future care and cooperation with clients. It reduces the probability of mistakes and lowers readmission levels. Second, it was assumed that the intervention is not too complex to require much time or sophisticated preparation. In such a way, it was expected that the offered project would work and promote positive outcomes.
The improvement strategy was implemented in phases. The first phase consisted of one-on-one training sessions for nurses on the importance of documentation and hands-on training on the hospital’s documentation system. The central hypothesis for this phase implied that prepared specialists might show better results, which is vital for the project. Furthermore, the strategy for change focused on altering nurses’ vision of CTAS and their attitude to documentation as the crucial part of working with clients. It was predicted that the training would lead to the desired outcomes, which was later proven by the results.
Afterward, nurses attended group sessions to discuss issues and share best practices. It was hypothesized that discussions might help to resolve problems if they remain and clarify issues that might influence results. The input from these sessions was used to develop the training curriculum. It was part of the change strategy to reconsider the current approach to working with clients using CTAS.
Concurrently, the IT staff concentrated on streamlining the system’s documentation process, reducing the number of steps required to enter data. Monthly evaluations were conducted to track progress and address any emerging difficulties. Mostly, the predictions coincided with the results as the discussions and interaction with the IT staff established the basis for the practical interaction.
As the strategy matured, it became evident that maintaining an open communication environment was vital to its success. Because their critique was not only recognized but also actively used to produce training and system improvements, the nurses felt empowered. This sense of ownership and engagement increased enthusiasm and commitment to the new processes.
The IT department’s proactive approach in working with the nursing staff meant that system updates were tailored to the actual demands of the users, making the documentation process more accessible and user-friendly. The strategy’s iterative structure, emphasizing continuous input and adjustment, ensured that the improvements were collaborative endeavors that resonated with the Emergency Department’s ground reality.
Findings
Data gathered following the intervention demonstrated a significant improvement in the timeliness and accuracy of vital sign documentation and CTAS evaluation.
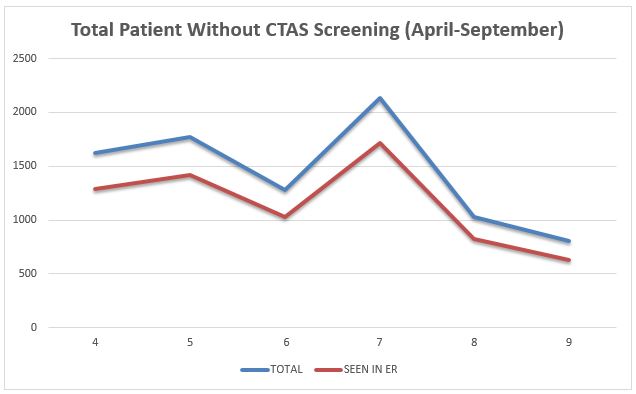
Figure 1 shows that gradually, the number of patients without CTAS screening reduced, which evidenced the effectiveness of training among nurses. Additionally, the total number of clients in ER departments also declined, which might result from using new interventions to work with patients, assess their vitals, report, and create the basis for enhanced care delivery.
Furthermore, the results demonstrated a large increase in the number of nurses documenting vital signs within the 15-minute window, as well as a significant drop in the number of times when repeating vital signs were not collected within 60 minutes. Contextual variables such as the reduced documentation procedure and continuing training sessions aided in achieving these results. There were a few outliers, usually owing to extremely high patient influx days or technical difficulties.
Comparing the results with baseline measurement, it is possible to admit a significant improvement. The number of nurses using CTAS and other interventions increased significantly, and almost all of them accepted the critical importance of the tool. This data evidences the importance of the intervention as the mechanism for reducing the number of readmissions and increasing the quality of care provision. Furthermore, the improvement compared with the baseline measurement means there is a potential for the further implementation of the tool to resolve various problems.
Aside from the numeric gains, there was a noticeable shift in the department’s attitude toward prioritizing documentation and patient triage. Nurses were confident in handling their jobs successfully, and inter-departmental communication improved noticeably. Feedback systems were also established, allowing for real-time modifications and guaranteeing that the imposed improvements were long-term sustainable. The project’s success was reflected not only in the figures but also in the improved morale and dedication of the nursing staff, highlighting the value of holistic approaches in healthcare quality improvement programs.
Several lessons were gleaned from this project:
- Continuous Training: The importance of continuous training cannot be overstated.
- Collaborative Approach: Engaging nurses in group discussions allowed for the sharing of challenges and best practices, fostering a collaborative environment where they could learn from each other.
- Technical Support: Having a dedicated IT support team was crucial.
The major strength of the project is using the healthcare setting with 40 workers who can share credible information about the current status of the problem. Additionally, it rested on data relevant data acquired from nurses and patients, which is critical for practical utility. The initiative, however, had its limits.
The sample size was limited to 40 nurses, which, while informative, may not be representative of other EDs. Furthermore, external factors such as patient volume and severity of situations on any given day may impact the documentation process, making consistency difficult to maintain at times. The main challenge was reaching nurses to acquire data from them and organize training. However, for new projects, a more structured approach with online interaction might be organized. It would simplify the process and ensure there is a platform to share ideas and interact.
Conclusion
Altogether, it is possible to conclude that it was a useful project with practical value. Using CTAS is one of the possible ways to improve outcomes, meaning educating nurses about it might promote positive change. The research attained its aims and investigated the problem using data provided by nurses. The selected measures were effective and helped to collect data effectively.
Furthermore, the discussed intervention might help to save costs for the healthcare sector by reducing the number of patients who need additional care and readmissions. It would compensate for spending on additional training and organizing the change within a selected unit. To ensure the work continues, it is recommended to select a more significant sample and analyze diverse settings that might require similar transformation. In conclusion, the project was a success that can be replicated by adding new components to continue the research in the field.
Reference List
McElroy T, Swartz N, Hassani K, Waibel S, Tuff Y, Marshall C, Chan R, Wensley D, & O’Donnell M. Implementation study of a 5-component pediatric early warning system (PEWS) in an emergency department in British Columbia, Canada, to inform provincial scale up. BMC Em. Med. 2019; 19(1). 74. Web.
Cotton R, Drew R, Douma M, O’Dochartaigh D, Keddie C, Muncaster K, Picard C. An analysis of individual and department tirage variances to identify, quantify, and improve markers of triage nurse accuracy. Canadian J Em. Nur. 2021; 44(2):19-20. Web.
Huy T, Lowrie L, Flood R, Chambers R, Weiss N, Nordike K, Wathen D. Improving the safety of an Emergency Department-Based Direct Admission process at a children’s hospital. Ped. Em. Care 2020; 37(12): e861–e865. Web.
Phaken C, Pearkao C, Potisopha W, Angkasith P. (2022). Evaluation of a web application for nursing records of multiple trauma patients in an emergency department. J of Em. Trauma, and Shock; 15(4): 167-172. Web.
Cox K, Lobell J, Champagne X, Lesko A, Corless L, Baraban E. Abstract TP249: collaborative in-person bedside handover improves emergency department nurses’ confidence in and compliance with documentation of frequent post alteplase neurological assessments. Stroke 2020; 51(1). Web.