Central Nervous System (CNS) associated disorders represent one of the major health issues globally. In this regard, the present description is aimed at highlighting a research proposal related to Posttraumatic stress disorder (PTSD).
Target Population Characteristics
The target population that is in dire need of change in behavior and/or health status is individuals who have Posttraumatic stress disorder (PTSD). The population being studied will be distinguished by the following demographic: African-American/European. The inclusion criteria for participants in the present study is:
- be male;
- self-identify as African-American/European
- be at a minimum age of 18 years;
- have had a history of PTSD related symptoms like anxiety, depression in the last 12 months;
- be drug adductors or abusers.
These individuals engage in several traumatic behaviors which may result in PTSD. These include war, terrorist attack, Sexual or physical abuse, Assault, Childhood neglect, Natural disasters and Sudden death of a loved one. (Smith & Segal, 2010). These behaviors may lead to anxiety disorder that is stimulated by the exposure to trauma (Meltzer-Brody et al, 2004). Individuals develop PTSD at a rate of one in four (Meltzer-Brody et al, 2004).
There is a need to identify individuals who require change in the form of remedy or rehabilitation from various corners of the health care. Earlier, a study described about women attending gynecology clinic. They were evaluated for their clinical history and hygienic conditions which revealed PTSD symptoms. It was found that majority of women were eligible for considering them under PTSD category (Meltzer-Brody et al, 2004). The demographic and ethnicity information reveled that they are African American with mean age of 34 years (Meltzer-Brody et al, 2004). Hence, the target population to be involved in this study would be African American women attending gynecological units at outpatient blocks (Meltzer-Brody et al, 2004).
The exclusion criteria will be set for those patients who are without PTSD symptoms.
Briefly this criteria includes:
- non African-American/NonEuropean;
- age below 18 years;
- had symptoms unrelated to PTSD.,
- have no history of drug addiction, abuse, assaults
- have not involved in acts that could have lead to trauma in the last 12 months.
Gnanadesikan, Novins and Beals (2005) reported about high risk PTSD individuals who are American Indian children and adolescents. These are found with variety of traumatic experiences and sexual trauma. Characteristics like age at first trauma, number of traumas, sex, kind of trauma are considered as they are associated with the PTSD (Gnanadesikan et al, 2005). In addition, they are also independent variables described to be associated with PTSD (Gnanadesikan et al, 2005). Therefore, identifying population characteristics is essential in the predicting the risky outcome of PTSD.
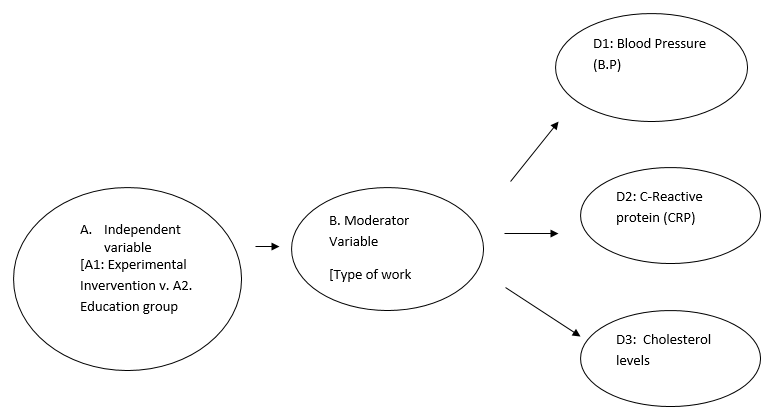
Independent Variable
In this study, the independent variable will represent two levels. The first will be the intervention being experimented and the second will be the education group. The first intervention that will be focused on PTSD management like cognitive-behavioral approaches like anxiety management, reprocessing, removing the sensation of eye movement, exposure therapy may improve the conditions of PTSD (Choi, Rothbaum, Gerardi & Ressler, 2010).
Cognitive-behavioral approaches like anxiety management, reprocessing, removing the sensation of eye movement, exposure therapy may improve the conditions of PTSD (Choi, Rothbaum, Gerardi & Ressler, 2010). In addition, NMDA agonist D-cycloserine, virtual reality-based exposure therapy were also proven to be important in ensuring the exposure therapy to ameliorate the efficacy of treating anxiety disorders and has implications for novel pharmacological developments in the area of behavioral therapy (Choi et al, 2010). The association between psychotherapy and the present pharmacological methods are significantly important for the success of psychosocial treatments (Choi et al, 2010).
There is a need to identify the flaws in the treatment interventions with regard to the psychodynamic therapy and anxiety treatments of hypnosis as they may contribute to inconsistencies on the efficacy of these treatment techniques (Choi et al, 2010).This has supported an earlier description on the treatment plans focused on posttraumatic stress disorder (PTSD). The second intervention is based on therapies like education oriented trauma management therapies. Here much emphasis was given on a spectrum of interventions that are frequently exploited in treating the patients with PTSD(Robertson, et al , 2004).These are cognitive therapy, trauma management therapy, stress inoculation therapy, exposure therapy, psychoeducation, hypnotherapy and psychodynamic psychotherapy(Robertson, et al , 2004).
Here the education will be focused keeping in view of strategies that are considered to improve the problem behavior or health status are dialectical behavior therapy, interpersonal psychotherapy, memory structure intervention, imagery rehearsal (Robertson et al, 2004). There is need to arrange 2 hour educational session to develop awareness for PTSD patients who present morbidity, and symptoms leading to decrease occupational interpersonal, and social adjustments (Robertson, et al, 2004). This program should be assonated with appropriate psychotherapeutic interventions without fail in connection with various modes of treatment under specialized treatment schemes (Robertson et al, 2004).
Moderator Variable
Type of Work atmosphere. This variable constitutes the influence of society actions on the behavior of victims susceptible for PTSD.
It was shown that male participants face severe work potential with negative appraisals of the world (Matthews, Harris, & Cumming, 2009). This would lead to the development of PTSD symptoms and altered cognitive coping(Matthews et al, 2009). Majority of the subjects were found with the symptoms of PTSD where there was diminished work orientation.
These subjects need encouragement about their self and worldly appraisals (Matthews et al, 2009). This may indicate that male individuals in a work atmosphere are more prone to PTSD (Matthews, et al, 2009).From the self-described trauma-related appraisals given by these subjects, it may indicate that PTSD is largely associated with the cognitive variables and work potential (Matthews et al , 2009). Therefore, PTSD management is dependant on coping strategies and Trauma-related appraisals that might influence the psychosocial behavior in male easily.
In contrast, PTSD symptom severity for women was found to be more than men. This could be because in college settings intimate relationships frequently get altered through abuses physically and sexually ultimately leading to posttraumatic stress (Avant, Swopes , Davis, & Elhai , 2010). Psychological abuse at the college level is a serious issue today and may have a negative emotional influence (Avant et al, 2010). PTSD outcome may be poor among certain college students but evaluating the psychological abuse is mandatory with regard to the earlier years of education in the colleges and the regulation of other factors like lifetime trauma history (Avant et al, 2010).
The research finings have revealed that in women trauma history is a god indicator of PTSD symptom severity compared to men (Avant et al, 2010). This could indicate that women pursuing college education may be more prone to PTSD and need to be largely screened (Avant et al, 2010). Thus, it is reasonable to mention that PTSD may influence males at the work place or females in colleges, which needs further investigation.
Dependent Variables
Blood pressure, C-reactive protein, cholesterol levels Next, it was described that PTSD is associated with the metabolic syndromes where blood pressure, obesity and insulin resistance play important role (Heppner et al, 2009).
Brunner et al described about the markers linked to stress-associated autonomic and neuroendocrine stimulation like high C-reactive protein, IL-6, blood viscosity, low heart rate(Heppner et al, 2009). This could be due to stress in the work place as noted earlier. This was revealed when a cohort of veterans have participated in a study where details on educational history, sociodemographic information and military service were sought in questionnaire(Heppner et al, 2009). It was found that moderating variables like serum triglycerides, high total cholesterol/HDL ratios were elevated (Heppner et al, 2009).
This has association with exposure to frequent loads of stress. Here, involvement of other factors like lifestyle, developmental and genetic factors were shown to be important in modulating the traumatic stressors.
This has strengthened the connection between metabolic syndrome and PTSD indicating that metabolic syndrome may serve as an important is a useful clinical indicator in influencing its quantitative effects on PTSD (Heppner et al, 2009). This may shed light on the need of important variables like body mass index and blood pressure which are more prone to deviation from the normal indices. Hence, the clinical outcome of PTSD could be largely dependant on these parameters.
Studies need to be carried out in evaluating the connection between PTSD and physical morbidity and mortality and examine whether there is concerted affects of metabolic syndrome on PTSD (Heppner et al, 2009). Therefore, moderating variables could be identified keeping in view of characteristics related to metabolic syndrome (Heppner et al, 2009). Here, apart from blood pressure, CRP levels, triglycerides HDL or LDL cholesterol levels also furnish better information. Basing on the conceptualizations described previously, a theory can be described. Firstly, a group of people from various ethnic or demographic regions need to be identified. The age of individuals is central to include in the study.
Recruitment at outpatient clinics is a good practice as they furnish information on gender, type and number of traumas associated with PTSD symptoms. The behavior of patients suspected for PTSD needs evaluation when cognitive skills deteriorate. This could be due to association of PTSD with the psychosocial functions. Equal opportunity for male and female participants is a mandatory factor while identifying the study characteristics.
This might positively influence the PTSD outcome. Variables help to asses the severity of PTSD. They could be dependant or independent variables. Drug addition may predispose an individual to PTSD through anxiety and altered behavior. It could disturb normal physiological process and corresponding variations in the dependant variables.
For example, drug addition may induce stress related symptoms like blood pressure alterations, increased hormonal production in response to stress. Here, interventions have great role to play. They have potential to assess the level of drugs in victims which furnishes insights on the severity of stress, previous exposure to violence, physical mental or sexual abuse and negative appraisal. This also reflects the type of environment the victim has chosen to work. Multiple studies would prove to be reliable in understanding the outcome of PTSD. Incidence reports may help to provide association with the drug and type of trauma.
It is likely that the PTSD victims arrested on the charges of drug abuse could revert back to the earlier life after release from the prison. Studies might prove beneficial when focused on memory structure intervention, interpersonal psychotherapy and dialectical behavior therapy. Costs associated with the PTSD vary significantly with the type or the severity of PTSD. For example, individuals who present PTSD along with depression require mental health drugs especially available and spent more compare to the depressed patients without PTSD (Chan, Cheadle, Reiber, Unützer, & Chaney, 2009). This could be due to the complexity of the problems associated with the PTSD (Chan et al, 2009).
Like PTSD patients with depression have mental health checkups at specialty centers, outpatient visits and have greater degree of emotional distress (Chan et al, 2009). They nee antidepressants in great quantity. Similarly, PTSD patients who have previously met with motor vehicle accidents also experience increased health and economic costs (Chan, Medicine, Air, & McFarlane,2003). This could be because motor vehicle accidents contribute to increased psychiatric consequences and medico legal and treatment aspects which are very closely related to posttraumatic stress disorder (PTSD) (Chan et al 2003).
Therefore, psychiatric disorders having deep connection with the motor vehicle accidents result in significant health and economic expenses quantitatively (Chan et al 2003). From the studies it was revealed that most victims were recognized with anxiety and others with depression (Chan et al 2003). In contrast, untreated PTSD patients experienced huge financial loss when compared with treated and non treated PTSD cases (Chan et al 2003).
This may indicate that treatment plans and severity of PTSD, its combination with other mental disorders greatly influence the financial burden to be incurred (Chan et al 2003). Therefore, the conceptualizations outlined here follow a sequence of information flow starting from the identification of characteristics on demographic and ethnic grounds, gender, drug addiction, and motor vehicle accidents. It is important to note that the outcome of a variable is largely dependant on the follow up period investigated by the health care professionals while assessing the severity of PSD.
The Theory of Causation
The Dependent Variables
Data Collection Procedures
The instruments being used for data collection will be the Clinician Administered PTSD Scale (CAPS).
It has a range between 0 and 136. This needs to used along with the Diagnostic and Statistical Manual of Mental Disorders, (DSM-IV) criteria. Most important variable blood pressure should be tested n combination with other physical tests like waist-to-hip ratio laboratory based 12-hour fasting lipids, glucose. While assessing hypertension, systolic and diastolic blood pressure values need to be united to reflect one condition.
Cut-off values should be utilized for high blood pressure, serum triglycerides, high-density lipoprotein, plasma glucose concentration. For PTSD data management, an accessor should seek information from the eligible participants.
Before this, a medical and psychological examination need to be conducted initially for the screening the subjects. Informed consent should be obtained such that the data can be utilized for other studies in the area of psychiatry. If the study is planned at University or Hospital, it needs approval from the concerned Institutional Review Board or Health care Department. Exclusion criteria should be followed for the participants, who do not present data from the any one of the variables under study, whose laboratory findings are not in agreement with the standard deviations (SD) from the group mean.
Similarly, those with very high laboratory findings should be excluded to facilitate efficient scrutiny of physiological burden on quantitative scale. These exclusion criteria would precisely yield the eligible participants. Sociodemographic information like educational history, military service and deployment (for veterans) need to be sought from the questionnaires. In addition, the questionnaire will assess and measure the following domains:
- demographics, anxiety, psychological distress,
- socio-cultural factors: type of work atmosphere, physical or sexual abuse
- developmental factors (perceptions of acquiring illicit drugs,
- alcohol and drug use;
- Trauma risk behaviors.
Measures related to PTSD severity like Clinician Administered PTSD Scale (CAPS), should be included. It has a range between 0 and 136. This needs to used along with the Diagnostic and Statistical Manual of Mental Disorders, (DSM-IV) criteria. Most important variable blood pressure should be tested n combination with other physical tests like waist-to-hip ratio laboratory based 12-hour fasting lipids, glucose. While assessing hypertension, systolic and diastolic blood pressure values need to be united to reflect one condition. Cut-off values should be utilized for high blood pressure, serum triglycerides, high-density lipoprotein, plasma glucose concentration. NCEP criteria should be followed for serum triglycerides and WHO and NCEP criteria should be followed for other parameters.
Here, although blood pressure is the important variable, its utility in connection with the severity of PTSD should be assessed in combination with other parameters. Finally, the important aspect of this description is about the threat measurement while collecting the data. A threat is a component that contributes to the outcome of the experiment. Here, there is need to describe about internal validity which is the treatment option that influences a dependant variable. The more the potential of an investigator to contribute to a change, the more will be degree of confidence that the intervention would lead to that effect.
The important threats to be considered for internal validity include testing, maturation, history, instrumentation, selection and experimental mortality. Therefore, while collecting the data emphasis should be given to year long reports on PTSD and related writing methodologies in a Hospital that may become erroneous by mismanagement. PTSD patients involved in long-term study on PTSD may show a decrease in the visits to a psychiatry clinic due to increasing PTSD cases instead of other treatment prescription.
Therefore, history and maturation may become more probably important for young individuals with PTSD and in longitudinal studies. Next, threat to measure is testing. To ensure the data quality, written formats and questionnaires need to be thoroughly evaluated for the kind of information to be sought, screening of PTSD patients at various clinical settings is important to enable the identification of perfect cases with significant study characteristics. Next threat to be measured is testing that result when changes take effect due to repeated testing instead of intervention. This issue is frequently encountered when the investigators come forward with the similar tests.
For example, PTSD patients need to be monitored for their behaviors, IQ’s and memory influenced by the prescriptions. When the physician or a doctor repeatedly prescribes the same drug or writes a questionnaire based prescription and obtains the similar results always, it could be due to earlier report on that particular strategy.
This would not demonstrate his or her natural habit of improved prescribing. Therefore, to ensure the quality of the data in this context PTSD based prescriptions should be changed according to the individual circumstances by the psychiatrist. The ultimate objective is to avoid repetition and try novel therapeutic strategies aimed at lessening the PTSD symptoms. The next threat to be measured while collecting the data is about the selection, PTSD patients referred from gynecology units receive should pharmacy-based educational intervention. Without this changes induced by the confounding variables like age, race, hysterectomy status, and menopausal status may become obvious.
To ensure the quality of the data on pharmacological interventions, relevant educational awareness programs need to be arranged for the PTSD patients. Similarly, experimental mortality is another threat that results due to a sudden cessation of experiment/treatment in advance without the completion of the experiment. PTSD investigations that are streamlined for the comparison of the anxiety drug effectiveness, for example, should take precautions that there is no loss of loss of subjects from the comparison that might lead to inequalities. Lastly, there is need to shed light on External validity which is emphasized on methodological procedures.
PTSD sample selection should be performed on random basis from the population. Otherwise characteristics like ethnic, racial, socio-economic, household, religious and/or income may become one sided partial and effect the outcome. Hence, sample collection process should be performed on a random basis. In view of the above information, PTSD is a severe anxiety disorder influenced by a spectrum of clinical characteristics that are dependant and independent. The relationships between Interventions and disease severity largely influence the outcome. Follow up studies might reveal significant information on many variables. An evidence based approach is necessary for the PTSD disease management and research modifications.
Table Design of the project depicting the interrelationships between the variables and outcomes related to PTSD
Design Table
References
Avant, E, M., Swopes, R, M., Davis, J, L., Elhai, J, D. (2010). Psychological Abuse and Posttraumatic Stress Symptoms in College Students. J Interpers Violence.
Brunner, E, J., Hemingway, H, Walker, B,R., Page, M., Clarke, P., Juneja, M., Shipley, M,J., Kumari, M., Andrew, R., Seckl, J,R, et al (2002). Adrenocortical, autonomic, and inflammatory causes of the metabolic syndrome: nested case-control study. Circulation, 106, 2659-2665.
Chan, A,O., Medicine, M., Air, T,M., McFarlane, A,C. (2003). Posttraumatic stress disorder and its impact on the economic and health costs of motor vehicle accidents in South australia. J Clin Psychiatry,64,175-81.
Chan, D., Cheadle, A,D., Reiber, G., Unützer, J., Chaney, E,F. (2009). Health care utilization and its costs for depressed veterans with and without comorbid PTSD symptoms. Psychiatr Serv, 60, 1612-7.
Choi, D,C., Rothbaum, B,O., Gerardi, M., Ressler, K.J. (2010). Pharmacological enhancement of behavioral therapy: focus on posttraumatic stress disorder. Curr Top Behav Neurosci, 2, 279-99.
Gnanadesikan, M., Novins, D, K., Beals, J (2005). The relationship of gender and trauma characteristics to posttraumatic stress disorder in a community sample of traumatized northern plains American Indian adolescents and young adults. J Clin Psychiatry, 66, 1176-83.
Heppner Pia, S., Crawford Eric F., Haji Uzair A, Afari Niloofar, Hauger Richard, L., Dashevsky Boris, A., et al. (2009). The association of posttraumatic stress disorder and metabolic syndrome: a study of increased health risk in veteran. BMC Medicine,7, 1-8.
Matthews, L,R., Harris, L,M., Cumming, S. (2009). Trauma-related appraisals and coping styles of injured adults with and without symptoms of PTSD and their relationship to work potential. Disabil Rehabil, 31, 1577-83.
Melinda Smith & Jeanne Segal (2010). Post-traumatic Stress Disorder (PTSD) Symptoms, Treatment and Self Help. Web.
Meltzer-Brody, S., Hartmann, K., Miller, W, C., Scott, J., Garrett, J., Davidson, J.(2004). A brief screening instrument to detect posttraumatic stress disorder in outpatient gynecology. Obstet Gynecol, 104, 770-6.
Robertson, M., Humphreys, L., Ray, R. (2004). Psychological treatments for posttraumatic stress disorder: recommendations for the clinician based on a review of the literature. J Psychiatr Pract, 10, 106-18.
Social Research Methods. Web.