Introduction
Family health assessment is an integral part of the healthcare practitioner’s activity. Health problems in general and chronic diseases, in particular, have an impact not only on a patient but on his or her family life as well. Health assessment demands skills and knowledge from healthcare practitioners to evaluate the health condition of family members and detect changes or abnormalities (Dains, Baumann, & Scheibel, 2015).
Family health assessment is conducted during a therapeutic conversation (Editorial, 2013). Such conversations proved to be efficient in improving family health (Persson & Benzeln, 2014). Wright and Leahey (2013) provide the Calgary Family Assessment Model (CFAM) which is “an integrated, multidimensional framework based on the foundations of systems, cybernetics, communication, and change theory and influenced by postmodernism and biology of cognition” (p. 47).
It includes structural, developmental, and functional categories which are divided into subcategories. However, not all subcategories should be studied during the first meeting. Their choice depends on the family and the situation and is the responsibility of a practitioner (How to apply the CFAM to clinical practice, n.d.). Thus, the following assessment is guided by CFAM and the selected subcategories were chosen after the consideration of family peculiarities.
Family Structure
Extended Family
The family which is the object of this assessment is a traditional one. There are six people living in one house. The father is 53 years old. He is an electrical engineer. His wife is 49 and she runs a small flower shop. She used to work as a nurse but the job was tiring and she worked shifts which did not leave enough time for the family, so she left her profession and tried a business that proved to be profitable. Her mother, a 78-year-old lady, lives with them. She is retired but active and helps her daughter in the shop and about the house.
The family has three children, two girls, and a boy. The elder daughter is 21. She is a student at a college and works part-time three days a week. On weekends, she works in the shop to let her mother have a day-off. The younger daughter is 19. She was adopted at the age of 2. She is at college, too. She also has a part-time job during weekends. The son is 14. He is at school and plays rugby for the school team. Sometimes he helps his mother in the shop with the delivery of flowers.
Medical History of Family Members
Patients’ complaints, present illnesses, past history, and family history are the components of health assessment (Bickey, 2013). The father was healthy until diagnosed with type 2 diabetes three years ago. He had an appendectomy at the age of 26. He did not report any other health problems. Moreover, after being diagnosed with diabetes, he has been following the diet and feels better at present. He was overweight but lost about fifteen kilograms during the three years of maintaining a healthy diet and his BMI is 27 at present.
The mother did not report any diagnosed diseases. She had two pregnancies which resulted in normal delivery. She had rubella at the age of five. The older lady demonstrates good health condition for her age. She has no signs of dementia and has an active lifestyle. Her activity is only limited by a cardiovascular disease that was diagnosed at the age of 63. However, she has been managing it successfully for fifteen years by now. The elder daughter does not have any serious health problems.
She is only allergic to oranges and some seafood, but it does not affect her life substantially. The adopted daughter had serious eye problems as a child. She was operated at the age of six. Although she is still visually impaired, her vision has not decreased since then. She has to wear glasses or lenses and control her vision. In addition, she has some activity limitations so as not to provoke vision loss. The younger son is healthy. He plays rugby for the school team. Thus, he regularly has examinations. His only problem is adolescent acne which is more cosmetic than medical. All children had smallpox in the early childhood (aged from two to four). Childhood illnesses do not have any effect on their health condition at present.
Sexual Orientation
All family members report being heterosexual. They were not engaged in homosexual relations. The older daughter shared she tried kissing another girl for a dare but did not like it.
Ethnicity and Race
The family is American. All of them were born and brought up in America. The older lady has French roots. Her great grand-mother moved from France to Canada and married an American. Later they moved to the United States and stayed there. All family members are white except for the adopted girl. She obviously has Latino roots. Probably, her mother or father was Latino. However, her biological parents are not known.
Social Class
The family belongs to the lower-middle class. The father is a wanted specialist and the mother runs a business, which is not big but profitable. They have had a house of their own for about fifteen years. Before that, they were renting one. After the mother left nursing and her business became profitable, they could afford to buy a house and invite the husband’s mother to live together. They travel around the country or abroad from two to five times a year depending on their activities and available money.
Religion and Spirituality
The family is religious. They are catholic and visit a church in the neighborhood on Sundays. They are not fanatic. However, they believe that church and faith help them to cope with complicated situations in life. Religion is also one of the forces which keep the family together. They report feeling inspired after their visits to the church or talks to the priest. The adult family members appear to be more religious than the younger ones.
Environment
The environment of the family is generally positive. Their house is in a peaceful neighborhood. It is a well-planned community with easy access to services or shopping spots. The family owns two cars. The parents and the elder daughter have driving licenses, but in case of necessity, every family member can travel by bus since public transportation is well developed in this area. Adults consider their neighborhood comfortable and perfect for life. The children do not deny comfort but report the lack of entertainment.
Family Developmental Stage
Stage of the Family Life Cycle
The family under consideration is in two stages of the family life cycle at the same time. On the one hand, it is a family with adolescents (stage) since their son is only fifteen years old. On the other hand, the elder girls aged nineteen and twenty-one put the family on stage 5 which is launching children and moving on (Wright & Leahey, 2013). Stage four for this family is not typical to the adolescent period.
Of course, it is emotional, but the son does not demonstrate delinquent behavior or the use of substances that are frequent in adolescence. The shift in parent-child relationships is gradual. The parents have some experience of dealing with adolescents although it was different from the girls. On the whole, the teenager’s growing up does not influence the emotional condition of the family.
Stage five which is also characteristic of this family is only beginning. Their grown-up daughters still live with parents although working part-time and having an opportunity to live separately. The elder daughter is going to separate after she gets married. The wedding is in half a year. The younger daughter is going to the university after she leaves college in a year and will live on campus. However, even when daughters leave, the son will still be in his teens. Thus, this stage will not be over for the next five or seven years.
Appropriateness of Developmental Tasks
One of the developmental tasks appropriate for this stage is “Shift in parent-child relationships to permit adolescents to move in or out of the system” (Wright & Leahey, 2013, p. 99). It is fulfilled in the assessed family. The boy has enough independence for his age. He selects hobbies, decides on his leisure activities, and has duties in the family. It proves that the shift mentioned above was made properly. The adolescent is independent enough and at the same time, he knows he will find support in the family.
Another task appropriate for this stage and clearly observed in the family is “Beginning shift toward joint caring for the older generation” (Wright & Leahey, 2013, p. 100). It is particularly suitable because a grandmother lives with the family. The boy is involved in helping his grandmother, one of his duties which was his initiative is accompanying grandmother to the church on Sundays.
As for Stage five, there are some developmental tasks appropriate for this family. First of all, it is “Development of adult–adult relationships between grown children and their parents” (Wright & Leahey, 2013, p. 101). Adult children in this family are rather mature and even have some financial independence. However, this task will be completed only after the girls begin their separate life. another task which is new for than family is “Realignment of relationships to include in-laws and grown children” (Wright & Leahey, 2013, p. 101).
It is reflected in the coming marriage of the elder daughter. As a rule, women can feel sad when their adult children marry and leave the family home. Nevertheless, in this family mother is more positive and the person who cannot reconcile with the perspective of the daughter’s status change is the father.
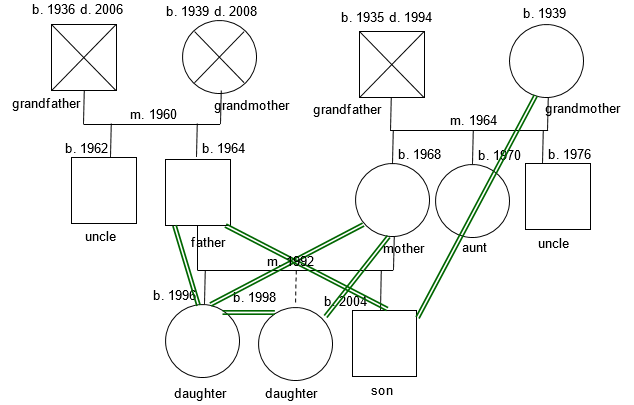
Genogram
Genogram provides an opportunity to get a broader picture of family relations and study the births, deaths, marriages, and other family events. It follows a certain structure and is a graphic representation of family life (Deena, 2013). The genogram of the assessed family can be seen in figure 1. It shows family connections starting from grandparents. Moreover, it provides a picture of attachment bonds in the family. It is evident that there is a strong attachment between the daughters and a mother while the son demonstrates an attachment to father and grandmother.
Family Functional Status
Family functional status includes the peculiarities of communication and interaction. It also depends on the ways of solving problems in the family. Moreover, it considers the family beliefs about life and illnesses.
Family Communication
Family communication includes its diverse aspects such as emotional, verbal, and nonverbal communication (Wright & Leahey, 2013). After the assessment, it can be concluded that this family is an emotional one. They are open and express their emotions freely. The positive aspect is that both positive and negative emotions can be expressed. It is equally acceptable to share happiness or express anger in this family. In the first case, the others will be happy too, in the second case, the person will find support and comfort.
Verbal communication is the major one for the family. Both oral and written, it is the way to transfer information, share news, or ask for advice. The tradition of the written messages in the family is a good way to wish a nice day or say something a person does not dare to say face to face. The observation showed that oral communication in the family includes a variety of topics. Family members demonstrate almost equal involvement in the communication process.
Nevertheless, daughters admit that they talk more to the mother than to the father. Nonverbal communication is also important for those people. They demonstrate intense eye contact which is the sign of openness. Moreover, they actively use gestures and facial movements, which are more typical of male family members.
Solving Problems in the Family
The skills of problem-solving are crucial for the family. This family follows the principle of dealing with the problem only when it arises. Moreover, the problem of one becomes the concern of the others. It became obvious after the father was diagnosed with diabetes. Since he did not realize the seriousness of the problem, in the beginning, both daughters and wife took care of him cooking proper meals and reminding to take medicine or visit the doctor. Due to such behavior, the disease did not become a problem but a change in lifestyle. The main role in problem-solving belongs to the parents, mainly the father. As the head of the family, he has the final say. However, the grandmother is the person who often is the crisis manager of the family.
Beliefs about Life and Illnesses
Beliefs of the family are the determinants of their functioning and behavior in different situations. In the context of the father’s illness, the family believes in good outcomes made them concentrate and find ways to adjust their life to new conditions necessary for the father. Although the family is religious, they do not believe diseases are a kind of punishment or trial. Even the grandmother who has been suffering from cardiovascular disease for fifteen years has trusted for medical science and eagerly takes her treatment or visits the doctor. On the whole, adult family members believe that illnesses are the result of their lifestyle or normal age changes and are ready to receive the necessary help.
References
Bickey, L.S. (2013). Bate’s guide to physical examination and history taking (11th ed.). Philadelphia, PA: Lippincott Williams and Wilkins.
Dains, J.E., Baumann, L.C., & Scheibel, P. (2015). Advanced health assessment and clinical diagnosis in primary care (5th ed.). St. Louis, MO: Elsevier Mosby.
Deena, S. (2013). Genogram instructions – marriage and family . Web.
Editorial. (2013). Family nursing is more than family centered care. Journal of Family Nursing, 19(4), 411-417. Web.
How to apply the CFAM to clinical practice. (n.d.). Web.
Persson, C., & Benzeln, E. (2014). Family health conversations: How do they support health? Nursing Health Research and Practice, 1-11. Web.
Wright, L.M., & Leahey, M. (2013). Nurses and families. A guide to family assessment and intervention. Philadelphia, PA: F.A. Davis and Company.