Calgary Family Assessment Model in Healthcare: Essay Introduction
CFAM (Calgary Family Assessment Model) is a tool utilized by health care specialists to evaluate the overall wellbeing of a family. It is concerned with the structure of the family, the interaction of the family members, their medical background, health status, and the environmental aspects that may influence the welfare of a family directly or indirectly. It allows a functional estimation of the family and enables providing guidelines how to improve the core functioning of it.
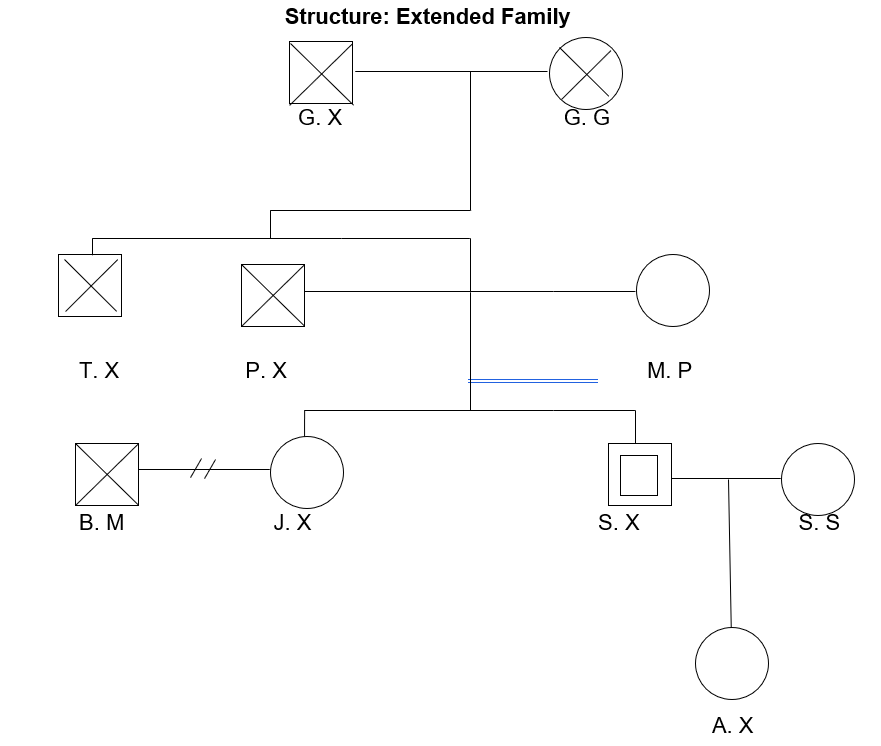
The CFAM was used to assess the family X. The family members gave their verbal permission for analyzing and compiling the evaluation of their family; however, their names have been omitted for the ethical reasons. The family members have been living in the United States; though, they originally come from Spain. They have lost connection with their other relatives when moving from Spain to the States and despite the fact that they made several attempts to make bonds with the rest of the family, they were incapable of doing so due to the reason that their relatives presumably moved to Finland. For that cause, the family is not aware enough of their medical history.
The family lives in Seattle, Washington, in the neighboring communities to be able to communicate with each other freely. At present, the family is not that extended due to several deaths that occurred during the past five years (Stanhope & Lancaster, 2014). S. X is a forty-nine-years-old male who lives together with his wife S. S. The couple has been married for almost fifteen years, and this is the only marriage for both of them. The couple got married in 2001 and gave birth to their daughter A. X one year after that. At present, A. X is thirteen. She will be fourteen in November. A. X lives together with her parents and studies at a community school. Every weekend she visits her grandmother and stays there for a sleepover. S. S is a forty-one-year-old female. The woman communicates with her mother-in-law that lives in the neighboring community. However, she does not know much about her relatives while she was raised in a shelter after both of her parents died in an accident. S. X and S. S are planning to have one more child next year if their family doctor approves of S. S’s health status.
P. X is S. X’s father that died two years ago at the age of seventy. P. X was ill with type 2 diabetes for ten years, though, he used to conduct an active way of life. He took prescription drugs, maintained a balanced diet and got the glucose level measured according to the treatment plan. However, during the last two years of life, P. X started leading a sedentary lifestyle and suffered from hypertension (Stanhope & Lancaster, 2014). J. X is S. X’s elder sister. She is fifty-years-old. J. X used to live with her husband B. M. They split up three years ago and now J. X lives with her and S X’s mother. She has no children of her own.
P. X had a brother, T. X, who died at the age of one for unknown reasons. M. P is S. X and J. X’s mother and P X’s wife. She is seventy-two and lives in the neighborhood. S. X and S. S visit her every week and her granddaughter A. X visits M. P every weekend. M. P has a deep bond with her family, and the connection between them has intensified after her husband’s health. The woman can be considered quite healthy (Wright & Leahey, 2012). She has some age-related health issues such as worsened eyesight, back pains, worsened memory; nevertheless, the woman takes the necessary blood tests and regular checks to monitor her health status.
G. X, S. X’s grandfather, was G. G’s husband. They got married when they were both twenty-years-old. They returned to Spain, and the family did not have an opportunity to keep in touch with them. They both died five years ago from natural causes. G. G died five months later after her husband did. Nothing else is known about the relatives as according to the family, they could not contact anyone after G. X and G. G’s deaths.
S. X visits their family doctor systematically as his father had type 2 diabetes, and S. X has increased sugar level and hypertension. He used to keep an imbalanced high fat and calorie diet, and he found out that he has increased levels of cholesterol and sugar in his blood (Stanhope & Lancaster, 2014). Since that time he regularly exercises and eats sufficient amounts of vegetables, in addition, he takes prescription drugs. At present, the man evaluates his health status as generally good. However, recently he has noticed that after workouts he feels discomfort in his knees and the sacrum area. The man links the pain to physical exercises, and he has decided to reduce the frequency and intensity of the workouts and substitute them with aerobic training. In addition, it was presumed that the drugs in combination with the aerobic exercises would enable controlling the blood pressure.
S. S claimed to have no chronic illnesses. Although, the woman used to have bad eyesight (hyperopia) and underwent an operation to restore it almost ten years ago. Moreover, the woman had appendicitis treated when she was pregnant. There were no complications in either the mother or the child (A. X) (Stanhope & Lancaster, 2014). The woman claimed to have occasional low-back pains; as per medical check, it is not connected to the organ malfunctioning. The woman appointed a check with the chiropractor. As it was mentioned earlier, S. S and S. X are planning a second child. The woman takes all the necessary lab tests and medical checks to exclude any complications related to the eyesight (possible retinal detachment) or musculoskeletal apparatus. Moreover, the latest blood sample evidenced a drop in hepatic parameters.
A. X has no acute diseases or chronic illnesses. The girl has a minor decrease in eyesight (-0,1), which is related to high school load (Burns et al., 2012). The girl visits a doctor on a regular basis to check her blood chemistry. The girl keeps a balanced diet, eats sufficient amounts of vegetables and jogs. Her health status is overall good.
J. X has hypertension as well as her brother does. She found it out after S. X was diagnosed with it. The woman takes medication and claims that she has no other health-related issues that would perplex her way of life.
As per B. M, his health was not discussed as he is not a member of the family anymore and B. M and J. X had no kids. As discussed earlier, P. X suffered from type 2 diabetes and hypertension. His health deteriorated during the last two years of his life. Until that time, he led an active lifestyle, kept diet, took his medication, and consulted his doctor according to the plan of care.
M. P is known to have quite good health. She has some age-related health issues (worsened eyesight, back pains, worsened memory); however, the woman contributes to her health status and consults the doctor regularly (Stanhope & Lancaster, 2014). Little is known about G. X and G. G as they moved to Spain and the family lost contact with them. According to S. X, both the grandparents suffered from hypertension that actively developed only during the last years of their life.
The members of the family are all heterosexuals. All of them are of Hispanic origin. Unfortunately, the family was not able to provide any further information about their ancestors because of the lost family connection. The described family belongs to the middle social class, and they are all Christians except for J. X, she is an atheist. The family honors Christian traditions and goes to church when they have such a possibility. The family tries to keep a warm relationship, and they are neighbors. J. X is a bit alienated from her family (Stanhope & Lancaster, 2014). S. X and S. S explained that it happened when J. X separated from her ex-husband. However, the family is quite united and socially active. The family attends social events and activities when they have time. Further, the family members are supportive of each other and tend to make joint decisions about crucial issues.
CFAM assessment: Family Developmental Stage
It should be noted that the family is on the fifth stage of development while making it through to the next level (Stanhope & Lancaster, 2014). Despite the fact that A. X is a teenager, she has almost no problems in communicating with the members of her family. In addition, she is close with her grandmother and helps her with the home chores. A. X’s parents are supportive of the girl; however, not overly protective. The parents allow the girl to make her own decisions regarding her hobbies and friends (Tomm, George, Wulff, & Strong, 2014). Nevertheless, there is a certain tension between J. X and the rest of the family while the woman prefers loneliness. However, she is not reluctant to help her mother when she asks her to and communicates with the family if the initiative comes from their side. S. X and S. S have joint interests and both take an active part in their daughter’s upbringing. The couple has a hobby (dancing), which they both like. M. P is also an active family member; she helps her son and daughter-in-law with A. X and has hobbies of her own.
The attachment bond between the family members can be characterized positively. It is secure and profound (Tomm et al., 2014). The family tries to involve M. P in family activities, show respect, and warm attitude to her through heart-to-heart conversations and family dinners. The family strives for making bonds with the other family members that presumably live in Finland. However, so far, they were unable to make contact with any of them.
CFAM model: Family Functional Status
Almost all of the family members are quite open and emotional. Their communication is meaningful, emphatic, and expressive. The verbal communication matches the non-verbal one (Bloom & Smith, 2012). Women of the family are more tempered; for that reason, S. X does his best to balance the moods and attitudes of the family members. No family members express disrespect or ignorance; however, A. X expressed her concerns that J. X is sometimes indifferent to her. The overall development of the family is effective as the family tries to improve the internal climate and considers each other’s feelings when discussing sensitive topics. In this regard, the circular communication is supported (Wright & Leahey, 2012). If any kind of misunderstanding is present, the family gives everyone a possibility to express his or her view on the problem. The family X executes a proactive approach (Bloom & Smith, 2012). They tend to consider the issue prior to taking any steps. If the situation requires thorough consideration, the family resorts to the family council. S. X took the role of the head of the family, and if they cannot decide unanimously, his opinion would be decisive. Nevertheless, in most cases, it is J. X that either starts an argument or expresses her indifference.
In conclusion, the family considers that an active way of life, healthy eating, and harmony within the family are the key aspects of physical and mental health. For that reason, they strive for an energetic approach towards everything and, if an illness occurred, they would take measures to cope with it effectively. Moreover, they do not reject traditional medicine if it is required and do not overdo it. The main principle of the family is that everything should be done in moderation, which is a rational approach towards health and the welfare of the family.
References
Bloom, M., & Smith, D. (2012). Brief mental health interventions for the family physician. New York, NY: Springer.
Burns, C., Dunn, A., Brady, M., Starr, N., Blosser, C., & Garzon, D. (2012). Pediatric primary care. New York, NY: Elsevier.
Stanhope, M., & Lancaster, J. (2014). Public health nursing. New York, NY: Elsevier.
Tomm, K., George, S., Wulff, D., & Strong, T. (2014). Patterns in interpersonal interactions. Abingdon, UK: Routledge.
Wright, L., & Leahey, M. (2012). Nurses and families. Philadelphia, PA: F.A. Davis.