Theory and Author Background
A nursing theory can be defined as a systematized understanding of phenomena that a nurse faces in his or her practice. The systematization is needed to ensure that nursing practice follows comprehensive guidelines in which the connections are explained between nurses’ activities and outcomes, such as ultimate quality of care.
The importance of theorizing in nursing has been recognized by scholars and practitioners within recent decades, as it has been argued that “[a] nurse increases professional power when using theoretical research as systematic evidence for critical thinking and decision making” (Alligood, 2014, p. 11). Apart from actual practice, the theoretical approach is useful in education and especially research because it allows students to develop analytical thinking skills when mastering nursing care and provides frameworks for new studies in the area that are aimed at improving the understanding and the delivery of nursing care.
Many nursing theories have been developed, and one of them is the comfort theory authored by Katharine Kolcaba (“Frequently asked questions,” n.d.). It is a middle range theory, which means that it is “a set of related ideas that are focused on a limited dimension of the reality of nursing” (Smith & Liehr, 2013, p. xiii). Compared to grand nursing theories, middle range theories are closer to actual nursing practice but still more theoretical than another category—nursing practice theories. In analyzing a nursing theory, it can be particularly useful to turn to the background of its author. Kolcaba is an Associate Professor Emeritus at the University of Akron’s College of Nursing (“Katharine Kolcaba,” n.d.).
She has been engaged in consulting for the College of Nursing and various health care institutions for many years, operating both nationally and internationally. Kolcaba graduated from St. Luke’s Hospital School of Nursing in 1965, received her RN/MSN degree from Case Western Reserve University in 1987, and received a PhD degree from the same university ten years later. She holds many awards, and one of the most remarkable ones is the Researcher of the Year from Sigma Theta Tau, the second-largest nursing organization in the world; she shared the award with Therese Dowd in 2006. Indeed, research is Kolcaba’s primary interest. Since the early 1990s, she has conducted many studies trying to collect new evidence supporting the theory or to test the theory in actual clinical conditions.
The theory remains influential, as many researchers from different areas of medical science and nursing care continue to use it in their studies. For example, Krinsky, Murillo, and Johnson (2014) used this theoretical framework in their study of patients who had symptoms associated with discomfort caused by cardiac syndromes, and the use of discomfort as a central concept in this study allowed the authors to provide practical recommendations on the basis of Kolcaba’s theory for promoting patient comfort.
Concerning the development of the theory, the central element of it was the exploration of different understandings of comfort, what constitutes it, what contributes to it, and what disturbs it. Since 1991, when Kolcaba first published her analysis of the concept of comfort, she continued her research in this direction and published a book in 2003 that remained the most cited of her works. However, since then, the author has conducted several other studies, most recent of which were dedicated to the application of the comfort theory to preoperative patients and patients with depressive disorders. Throughout Kolcaba’s works, the main concern addressed by her theory is still the attempt to establish what causes patients’ discomfort and what promotes their comfort.
Theory Description
In analyzing a theory, it is important to address the direction of theorizing, i.e. whether the theory employs deductive, inductive, or retroductive reasoning. Deductive reasoning is moving from general principles to specific conclusions; inductive reasoning is moving from specific examples to general conclusions; and retroductive reasoning is explaining a phenomenon by premises that do not necessarily entail it. However, pure deductive, inductive, or retroductive approaches are rarely applied to complex real-life phenomena because such phenomena require complicated analysis that can involve different types of reasoning. The comfort theory is an example of such analysis because it addresses a rather challenging concept of patient comfort that can be explored and explained in various ways.
On the one hand, the comfort theory uses inductive reasoning because the basis of this theory is observing patients in actual clinical conditions. By collecting patients’ feedback and attitudes toward what constitutes their comfort and causes them discomfort, Kolcaba constructed a set of systematized specific examples that were further analyzed to create a theoretical framework and a theoretical understanding of patient comfort (“Frequently asked questions,” n.d.).
However, on the other hand, it can also be said that deductive reasoning was used, too. In their discussion of the comfort theory, Smith and Parker (2015) note that it is popular because “it describes what expert nurses already know: One of the most important missions for nursing is still to bring comfort to our patients and families, no matter what their circumstances are” (p. 390). Therefore, the theory uses generally known principles as the foundation for its systematization of findings, and this approach allows establishing that deductive reasoning is used because the use of premises that are known to be true for further specification of concepts is a sign of deductive reasoning.
The comfort theory’s essence is the description of the relationships among patient comfort-related concepts identified by Kolcaba. These relationships are shown in Figure 1.
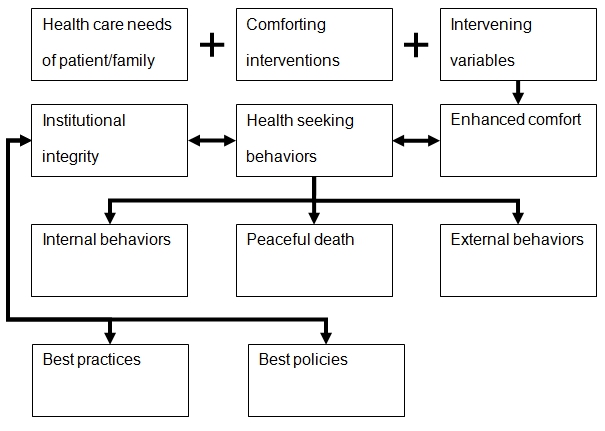
As seen from the conceptual framework above, the comfort theory operates several concepts that were not initially created for this theory; however, it should not be neglected that definitions used by Kolcaba may be somewhat different from what other authors may mean by the same concepts. Major concepts of the comfort theory are the three contributors to enhanced comfort: health care needs of patient/family, comforting interventions, and intervening variables. An important aspect of the first concept is that the needs are identified by patients and their families, not by a nurse, and further communicated to him or her.
This is important because, in some theories, it may be suggested for a nurse to establish the needs of a patient on the basis of observing the patient; in the comfort theory, instead, it is suggested to pursue the needs as defined by patients and families. Further, along with comforting intentions that are inevitably present in any guidelines on how to enhance a patient’s comfort, Kolcaba includes the concept of intervening variables that she defines as “factors that each patient brings to the health care situation, that nurses cannot change, and that have an impact on the success of the interventions” (“Frequently asked questions,” n.d., para. 17), i.e. such factors as the financial situation of a patient or the level and form of social support.
The most important concept of the theory is comfort itself, and Kolcaba defines it as “the immediate experience of being strengthened through having the needs for relief, ease, and transcendence” (“Frequently asked questions,” n.d., para. 2) and argues that comfort is, in fact, a primary desirable outcome of nursing care. It is stressed that consistent delivery of comfort interventions will cause desired health seeking behaviors in patients and will improve institutional outcomes. Among health seeking behaviors, the author distinguishes between internal ones (what a patient is like, e.g. immune system, healing, and physiological characteristics) and external ones (what a patient does, e.g. health-related activities and everyday practices). Concerning the concepts that are affected by and affect institutional integrity, Kolcaba defines best policies as evidence-based protocols developed by a health care institution and best practices as evidence-based procedures for specific patient application.
The definitions of terms are mostly explicit, as Kolcaba pursues clearly explaining everything that she thinks is relevant to the conceptual framework. However, the definition of comfort itself is rather implicit because the theory’s author does not define comfort definitely but instead suggests treating this concept as something that encompasses a wide range of considerations related to successful and effective delivery of care and positive patient experience.
Evaluation
The entire comfort theory, as seen from the definitions it operates (see Theory Description), is built on the basis of the assumption that providing comfort to a patient is a major purpose of health care delivery. This is important because not all theories list patient comfort among primary purposes of care. For example, it can be argued that the main goal of a medical team is to ensure that treatment provided to a patient causes positive health outcomes despite the fact that it may cause the patient discomfort, too. It should be acknowledged that any intervention is inevitably a factor that contributes to discomfort, and this is exactly why Kolcaba suggests approaching the process of treatment as something that requires constantly ensuring that patients’ needs are properly addressed and support is provided so that patients do not feel lost, desperate, and depressed; otherwise, the health outcomes of treatment cannot be considered fully positive.
In evaluating a nursing theory, it is useful to discuss its metaparadigm, i.e. a set of universal concepts to which any other nursing theory inevitably refers. Here, “universal” means that these concepts are applicable across nursing theories in various contexts; however, it does not mean that these concepts have universal definitions. In fact, different theorists may suggest different definitions for what they all refer to, i.e. such concepts as health, patient, and care. Kolcaba specifically defines four metaparadigm concepts. First, nursing is defined as “the intentional assessment of comfort needs, design of comfort measures to address those needs, and re-assessment of patients, families, or community comfort after implementation of comfort measures, compared to a previous baseline” (“Frequently asked questions,” n.d., para. 11).
Second, a patient is defined as an individual, family, or community that requires care. This definition implies that the need for care is the sufficient and most important criterion for qualifying a person for a patient, and not only a person can be qualified as such but also families and communities. Third, environment is defined as a set of external factors that include physical settings as wells as policies and institutional support. Fourth, health is defined as the optimal way of functioning of a patient, and, interestingly, the concept of comfort is incorporated into this definition, as Kolcaba claims that proper attention to comfort needs is what facilitates health.
Concerning the consistency of the theory, it can be said that some elements of Kolcaba’s metaparadigm are somewhat confusing. For example, it is not explicitly explained why a family or a community can be regarded as a patient. In patient-centered care, an individual is the main focus of health care provision, and it is acknowledged that proper attention should be paid to the patient’s family and community because they constitute the environment of the patient, the context of treatment, and the source of necessary support.
But it does not mean that a family can be treated as a single patient, while Kolcaba’s definition implies that it can. Besides, Kolcaba repeatedly uses the words patient/family/community written with slashes, and this is confusing, too, since her definition of a patient already includes family and community. However, shifting from the metaparadigm to the conceptual framework of the theory, it can be said that the concepts are more consistently defined, which increases the validity and reliability of the theory.
Application
The most obvious and immediate application of the comfort theory to guiding nurses’ actions is that promoting comfort should be pursued as the main goal of nursing care. Based on Kolcaba’s definition of comfort, there are four contexts of experience for meeting the patients’ need for comfort: “physical, psychospiritual, social, and environmental” (“Frequently asked questions,” n.d., para. 2). The physical context describes how a patient feels, i.e. refers to physiological functions and processes, and what a patient feels, i.e. refers to sensations and experiences associated with treatment and staying in hospital.
The psychospiritual context describes the extent to which a patient is aware of his or her state and how he or she understands the encountered health problems and treatment. The social context, also known as the sociocultural context, describes the patient’s relationships, both interpersonal and societal. The environmental context describes external surroundings of the patient but, unlike the physical context, it also includes the atmosphere, the attitudes of people around the patient, and the support the patient receives. These four contexts are the areas in which a nurse should act to enhance comfort.
According to the comfort theory, in practice, a nurse should identify the needs of a patient—by communicating with the patient rather than independently and based on observations (see Theory Description)—and divide them into the four contexts described above. This course of action is justified by the recognition that interventions needed to meet the needs in different contexts are different.
Enhancing patient comfort in the physical or environmental context may require introducing certain adjustments in the patient’s room and communicating with the physician, e.g. in case a patient experiences severe unceasing pain, and an increased dosage is needed, or with the administration of a medical facility, e.g. in case a nurse wants to recommend an amendment to existing patient-related policies. At the same time, enhancing patient comfort in the psychospiritual or social context may require extensive communication with the patients’ families or patients themselves. By adopting this strategy, a nurse will ensure that comfort is a priority, and the overall quality of care, according to Kolcaba, will be thus improved.
References
Alligood, M. R. (2014). Nursing theorists and their work. St. Louis, MO: Elsevier.
Frequently asked questions. (n.d.).
Introduction. (n.d.)
Katharine Kolcaba. (n.d.)
Krinsky, R., Murillo, I., & Johnson, J. (2014). A practical application of Katharine Kolcaba’s comfort theory to cardiac patients. Applied Nursing Research, 27(2), 147-150.
Smith, M. C., & Parker, M. E. (2015). Nursing theories and nursing practice (4th ed.). Philadelphia, PA: F. A. Davis.
Smith, M. J., & Liehr, P. R. (Eds.). (2013). Middle range theory for nursing (3rd ed.). New York, NY: Springer.