Statement of the Position
The discussion was about the National Health Insurance (NHI) system while showing its potential influence on the development of the policies. The position of our group states that the NHI could be considered as a major source of the drawbacks associated with low reimbursement, lack of efficiency, and the absence of inclusiveness while questioning the freedom of choice. This paper represents the flow of discussion and summarizes the outcomes in the conclusion.
Argument 1
The opponent claimed that one of the benefits is access to care, as it forbids the insurance companies to deny the coverage of the patients (Estes, Chapman, Dodd, Hollister, & Harrington, 2013). Meanwhile, the opposing team also stated that this program ensures the coverage of the low-income segment while cultivating the growth by 60 percent, cost-efficiency, and the minimization of discrimination (Chiplin & Lilly, 2013). In response, our team claimed the NHI might be prejudiced and depicted that discrimination associated with education is more likely to occur (Newhouse & McGuire, 2014; Odeyemi & Nixon, 2013) (see Figure 1).
The lack of inclusiveness was highlighted as a counterargument, as some of the population groups are being ignored, and the barriers related to the lack of education and information prevent the patients from making the right choices (McDoom, Koppelman, & Drainoni, 2012; Newhouse & McGuire, 2014). In this case, one of the examples is the fact that women experienced lower coverage rates in 2011 (especially widowed and retired) (Salganicoff, 2015).
Argument 2
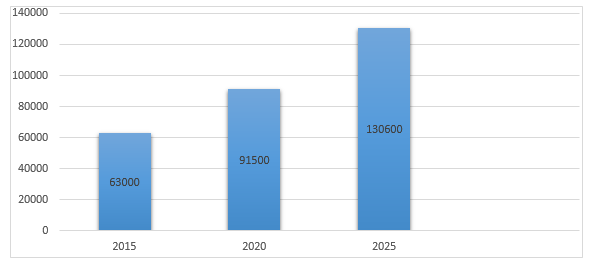
The second claim of the opponent was related to the rising healthcare expenditure and the possibility of the NHI to reduce it (Bodenheimer & Grumbach, 2012). Meanwhile, it was determined that the United States has the highest spending in this sector in the world (Hockenberry & Thorpe, 2014). Our group agrees with the opinion, as the number of insured patients increased to 30 million people elevates the overall expenditure (Bodenheimer & Grumbach, 2012).
Nonetheless, the usage of the NHI will not reduce this matter, as the extended control of the government will decrease the overall number of doctors due to the rise in the number of patients under the ACA (Addressing the physician shortages, 2011). In this case, our primary argument was connected to the issue of reimbursement rates, as this matter is highly associated with discrimination while leading to the increase of the healthcare costs (McDoom et al., 2012; White, 2013).
Argument 3 and Argument 4
As for the subsequent argument, the opponent refers to the increased affordability of healthcare, as it offers individual adjustment of the required payments based on the personal salary (Society for Human Resource Management, 2016). Another argument for the application of NHI is the usage of the concept of the global insurance plan model, as it implies that the current US insurance system is more expensive while comparing it to the UK. The counterargument to this statement is the fact that the taxes will double as the comparison of the UK (37%) and the US (15.3%) taxes emphasizes the differences in payroll (Gregory, 2013).
As for the arguments against the NHI, a new policy is highly criticized, as it failed to increase managed care plans (Newhouse & McGuire, 2014). The introduction of the NHI questions the freedoms of individuals, as it limits their choices (Cohen, 2015). These concepts underline that improvement is a necessity.
Argument 5
Lastly, the opponent states that the implementation of the novel insurance system will improve the quality of healthcare and uses the example of the UK and Canada and their increased satisfaction rates (Bodenheimer & Grumbach, 2012). On the contrary, our group suggests that the definition of happiness and questionable, as the UK healthcare service includes long waiting lists while depicting that 12% of the population is using private plans despite the high prices (Odeyemi & Nixon, 2013) (see Figure 3).
Meanwhile, the argument of our group emphasizes that the 2010 Patient Protection and Affordable Care Act increased the coverage of the elderly to 30 million people while being a driver for the increased efficiency of the services (Bodenheimer & Grumbach, 2012). Nonetheless, the organizational structure and the quality of the services is still a problem, and new policies have to be proposed to improve the excellence.
In turn, the opponent provides the example of the comparison of two studies, which were used to highlight that the pay for performance system gained success in the UK among the physicians, and the metrics system was implemented (The Kaiser Family Foundation, 2015). On the contrary, our group revealed that it is difficult to access the quality measures and highlighted the possibility of manipulations (Ryan & Damberg, 2013; Bodenheimer & Grumbach, 2012). Lastly, our group provided a VPN as an example and highlighted the difficulties in monitoring the results (Ryan & Damberg, 2013).
Conclusion
The discussion was heated due to the paramount importance of the topic in modern society. Despite the active usage of the statistical and factual information to support the necessity of the NHI, our group won the discussion, as we were able to provide specific examples while combining them with the persuasive argumentation. The outcome of the debate was predictable, as the group prepared the rebuttals to the arguments of the opponent by using additional literature, statistics, and a well-developed structure of the sentences.
References
Addressing the physician shortages under the ACA. (2011). Web.
Bodenheimer, T., & Grumbach, K. (2012). Understanding health policy. New York, NY: McGraw-Hill Medical.
Chiplin, A., & Lilly, B. (2013). Medicare’s future: Letting the affordable care act work, while learning from the past. National Academy of Elder Law Attorneys, 9(1), 123-135.
Cohen, J. P. (2015). Implementing the affordable care act: Remaining hurdles. Clinical Therapeutics, 37(4), 717-719. Web.
Estes, C., Chapman, S., Dodd, C. Hollister, B., & Harrington, C. (2013). Health policy crisis and reform. Boston, MA: Jones & Bartlett Learning LLC.
Gregory, P. (2013). Obamacare a mess? Liberals say go single player. Forbes.
Hockenberry, J., & Thorpe, K. (2014). Slow health care spending growth moderates GDP growth in the short term and policy targets should reflect this. health affairs blog. Web.
McDoom, M., Koppelman, E., & Drainoni, M. (2012). Barriers to accessible health care for Medicaid eligible people with disabilities: A Comparative analysis. Journal Of Disability Policy Studies, 25(3), 154-163. Web.
Newhouse, J., & McGuire, T. (2014). How successful is Medicare advantage? Milbank Quarterly, 92(2), 351-394. Web.
Odeyemi, I., & Nixon, J. (2013). The role and uptake of private health insurance in different health care systems: are there lessons for developing countries?. Clinicoeconomics and Outcomes Research, 5, 109-118.
Ryan, A., & Damberg, C. (2013). What can the past of pay-for-performance tell us about the future of Value-Based Purchasing in Medicare? Healthcare, 1(1-2), 42-49.
Salganicoff, A. (2015). Women and Medicare: An unfinished agenda. Generations, 39(2), 43-50. Web.
Society of Human Resource Management. (2016). Payroll Tax unchanged: tax brackets nudge up. Web.
The Kaiser Family Foundation. (2015). Primary care providers’ views on recent trends in health care delivery and payment. Web.
White, J. (2013). The 2010 U.S. health care reform: Approaching and avoiding how other countries finance health care. Health Economics, Policy and Law, 8(3), 289-315. Web.