Almalki, Fitzgerald & Clark (2011) stated that the policymakers and researchers are working with the healthcare industry of Saudi Arabia and they suggest to introducing gradual privatization of the health care services at public sector hospital; however, the government has already passed relevant law to put into practice of the privatisation strategy.
The policymakers argued that privatisation would reduce governmental expenditure rather it would reduce complexities of decision-making at the governmental hospitals and the quality of service would improve pointing to the market demand, motivating with such idea, a number of governmental hospitals have already sold to the privates sector and the others are given to the private operators by rent. Theoretically, it is seemed that privatisation would speed up medical service by generating perfect competition, government would be beneficial from two sides first one is deducting the public health expenditure and the second one is as a new source of financing the ministry of health.
At the same time, it is also argued that privatization would seriously impact on the existing Hospital management and the scope of Primary Health Care, after the privatization, it would create lacking in the patient nursing, treatment facilities, medicine, along with the PHC services, which is a community hospital that could refer the patients to the big hospitals.
As a result of privatization the community health care would also be hampered, citizens have to pay high cost for medical support; state service to the people would reduce and the profit-making trend would rise rather than welfare service to the distressed people. On the other hand, the private companies are not interested to go to the rural areas, thus, government of Saudi Arabia needed to make certain regulation that would ensure public health service to the small and indigenous communities at remote areas of the country.
Current health system in Saudi Arabia
Ahmed (2013) conducted a landmark study with the present status of healthcare sector of the Kingdom of Saudi Arabia and pointed out that around 60% of the hospitals and diagnostics in KSA have built, owned and operated by public sector under the Ministry of Health (MoH) those consist with basic healthcare facilities along with specialised treatment. The Ministry of Health (MoH) has been keeping continuous efforts to boost the medical facilities for the Saudi people, the existing facilities allow only local people to get state facilitated medical services for specialised treatment, but there is no easy access for the expatriates working in the county.
The foreign workers working Saudi Arabia are almost half of the population and accounted about 9.0 million, for primary healthcare to specialised treatment they are forced to take healthcare services from the high paid private hospitals although some organisations have their own free medical facilities for their workers, but that is very limited. The state employees such as defence service, police, national aviation, and the employees of Royal Commission are entitled to get full free medical service from the governmental hospitals as well as from the private sector if required
Although Saudi Arabia is one of the riches countries in the world, its spending for public health is very poor in relation to the other developed economy; the statistical data of the country illustrated that t allocates 3.7% of the GDP medical service while the USA spends 17.9% of the GDP and UK spend 9.3% for public health.
With a population of 26 million and 2.2% growth rate the governmental spending is not satisfactory and the police have not yet settled how the country would encounter with the rising needs of public service in the healthcare sector while MoH is the owner of 60% hospitals in Saudi Arabia. Beside the Ministry of health, there are some quasi-governmental organisations those provide healthcare service to the vital state employees, due to lack of easy access to governmental healthcare, the private investment in this industry is continuously increasing and the overall public health is under serious risk with the rising cost.
Public Health Policy and Ongoing Programmes in Saudi Arabia
WHO (2013) pointed out that the prime health care service provider is the Ministry of Health and it had designed the national 5-year development plans in 1970 and reviewed these plans time-to-time in order to focus on different issues, for instance, 8th NDP revised in 2005 to offer better services to the citizens of KSA. According to the report of WHO (2013), the government of this country has already enhanced health care sector particularly numbers of service centres was raised by 8.90% from 2004; in addition, health care indicators demonstrated that vaccine-preventable diseases along with mortality rates had decreased significantly within the last decade.
Subsequently, the policy-maker of this country had introduced ninth NDP from 2010 to 2014 to enhance health care sectors; furthermore, the policy has developed with intend to address the demand of the people (Ministry of Economy and Planning 2010, and WHO 2013). The ninth NDP has provided policy grounds to implement in the health care sector; however, these grounds include:
- The main objective of this plan is to increase number of sources of funding for health actions; however, it focused on the Cooperative Health Insurance Scheme, civil charities, the waqf and the state budget as good sources of financial support to ensure public health care service (Ministry of Economy and Planning 2010, and WHO 2013);
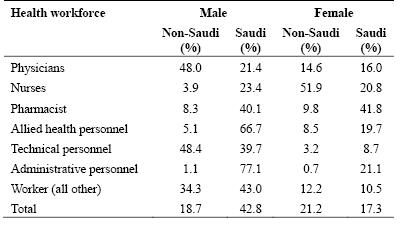
- Improvement of information technology to support information systems in the health segment is one of the main goals of this plan; in addition, it concentrates more on proper management and operation systems by decentralizing administration and arranging separate budgets for this sector (Ministry of Economy and Planning 2010, and WHO 2013). At the same time, the policy makers intend to decentralize management to ensure quality and standards in health services and to implement proper health care strategy; however, the following figure shows the percentage of Ministry of Health workforce in 2009:
- The government and other decision-makers of this country had designed public health policy to reduce the burden of chronic non-communicable diseases, control population growth and fertility rates, prevention of genetic disorders (inherited blood diseases), develop awareness to prevent female diseases and so on;
- In addition, the policy makers focused more on the reduction of non-communicable diseases as more than 71% people died in KSA for these diseases
- Decrease dependency on the expatriates and increase national staff and specialist in this sector to develop efficiency level; at the same time, it decided to strengthen the private health sector besides public health services to increase effectiveness to serve the whole population (Ministry of Economy and Planning 2010, and WHO 2013).
- The government of KSA will take different initiatives in order to enhance the emergency medical services with intent to save the people at the time of disasters (Ministry of Economy and Planning 2010, and WHO 2013);
- This plan included other relevant issues such as safe handling of medical waste, energy and water usage, monitoring, and control over production, strengthen inter-sectoral collaboration at the sub-national level, develop curative care in four curative levels, and ensure balanced distribution of health services for the citizens of KSA and so on.
Consideration of impact to citizen
It is highly important at this stage of the paper to consider the impact of privatisation of health insurance sector over the citizens of the Kingdom of Saudi Arabia. The medical care scheme in Saudi Arabia ascertains medical coverage without charge for every citizen and emigrant in public division; this is due to reason that regulations of the country want every citizen to be entitled to free treatment; moreover, private division workers get fundamental medical coverage from their employers in form of insurance procedures offered by private insurance businesses.
Private medical insurance scheme in Saudi Arabia emerged because of the execution of the Health Insurance Act (1999); it intends to manage and adjust the condition of medical insurance for both Saudi citizens and for foreigners who stay here as expatriates; however, it is notable that since the execution of the Act, massive privatisation of the medical insurance sector occurred. It has been reported that this advancement has proven to be highly advantageous to the citizens of the Kingdom of Saudi Arabia, for example, by increasing competition among the companies offering the insurance policies and in turn benefiting people with superior and high quality services.
Consideration of impact to Government
Eljelly (2009) conducted a landmark study with the listed governmental companies, listed private companies of the Kingdom of Saudi Arabia, and identified that the privatisation increases management efficiency, less complexity of decision-making, higher retune on investment and mostly outperform in context of governmental ownership- it is the general motivation of the privatisation theoreticians.
On the other hand, due to WTO membership and signing GATT, the country is continuous under pressure to accelerate its privatisation drive, but a closed society like KSA has to face very difficult shock to drive to the open economy complying with the terms and condition membership. Bagaresh (2013) added that KSA as the biggest oil producers in the world with its strong religious values, forbidden products, and unchallenged monarchy has been struggling to implement ruthless privatisation strategy with the aim to integrate itself with the world economy, that producing serious pain for the economy in order to share burden of the US banking sector collapse
Role of WHO
WHO (2013) reported that the main medium-term objective of this institute is provide technical support under CCS process to the government of KSA; in addition, this organisation has identified health priorities and challenges after scrutinising the health situation considering a holistic approach. In addition, this institute assists the policy-makers and government to set up health policies by take into account socioeconomic status; it designs framework of 4-6 years to develop health system; however, the government of this country considers the suggestion of this institute to achieve the Millennium Development Goals (WHO 2013).
At the same time, this institute recommends the government of this country to focus more on the public health sector privatization in order to develop performance and quality of the services; however, WHO established a collaborating centre in this country to give technical assistance to develop high quality specialist expertise through training, scientific research, and other activities.
Compulsory Medical Insurance in Saudi Arabia
CHIC (2009) pointed out that a Ministerial Decision in 2009 has introduced the Cooperative Health Insurance Law in the Kingdom of Saudi Arabia aimed to implementing compulsory medical insurance for the employees and individuals in the kingdom in order to safeguard their life from unexpected accident, impulsive injury and unanticipated events taking place within the insured the period. The Article-2 of the ‘Cooperative Health Insurance Law’ illustrated that the expatriates Saudis employed in the private sector, unemployed residents, individuals under labour contracts have to maintain compulsory medical insurance for their own as well as fro their family members and dependents live in the Kingdom of Saudi Arabia.
On the other hand, expatriates working in the governmental agencies of Saudi Arabia and has no provision to getting healthcare services into their work contract, the employment authorise are be obligated to provide them insurance facilities that they willing to get in accordance with standard insurance policies available in the local market. Family members of such employees would get similar insurance coverage for their treatment with similar quality and standard under the Cooperative Health Insurance Law’.
Under the Cooperative Health Insurance Law, the employers have to choice a health insurance company from where they take insurance coverage for all the employees within the organisation, at the same time, all new employees are also mandated to get similar insurance facilities under this law. Private medical companies who provide free medical check up facilities for their employees may not be exempted from the compulsory insurance coverage to their employees.
It has instructed to the insurance companies to issue a binding over the expatriate employees to check the renewal copy of the residence permits, if it is not renewed the policy would be cancelled and the companies would timely inform such issues to the CHIC to keep in record for further reference. In case of switching jobs, the new employers would be liable to provide similar premium to continue the insurance policy with out any hindrance, the employers also authorised to changing insurance companies with a notice of one month.
The objective of the Cooperative Health Insurance is to ensure funding to cover all expenditure of treatment and medical facilities pointed in the insurance policy including the cost of procedures and controls of CHIC activities together with its financing with identifying beneficiaries corresponding with SAMA. CHIC has other financial resources such as collecting application-processing fees, which is 1% of the total premium collected by the insurance companies, annual renewal fees of the insurance company and claims management agencies working in the kingdom, the Cooperative Health Insurance Council has also income from different publications, while it also recognised to take donations, and grants including investment revenues.
Impact of Compulsory Medical Insurance on the Citizens
Ahmad (2011) conducted a landmark study with impact of changing dynamics of the insurance industry in Saudi Arabia based on secondary data of SAMA, assessing the industry performance before and after the introduction of compulsory medical insurance in the kingdom and pointed out that the impact of reforms on the standardization by regulatory framework has made significant progress. During the reformation of insurance industry from 2004 to 2009, has explored the door of insurance market for small, medium and large insurance companies from the local and foreign countries and demonstrated significantly higher growth of premium with remarkable penetration of indigenous companies in the KSA market.
For the last two decades, the world insurance markets has evidenced a robust growth in the history, from 1997 to 2004 the aggregate market growth recorded 82%, where real premium of life insurance boosted 102% and the non-life growth was recorded 60%, the real premium jumped from US$ 1.6 trillion towards US$ 2.9 trillion. With in this period, Saudi Arabia came into agreement and signed membership of WTO, at the same time the country integrated with WHO, as a result the KSA could not keep itself out of the global market dynamics.
Thus, the introduction compulsory medical insurance in Saudi Arabia has dramatically increased the growth of real premium both in life insurance and in the non-life segment and enhanced the overall economic growth by generating new employment opportunities, large fund mobilisation, and enhanced social safety net for the local people and the expatriates.
Furthermore, the opening of compulsory medical insurance in Saudi Arabia has dramatically influenced the financial service sector and remarkably enhanced economic performance in every sector by boosting trade and commerce, increasing number of institutional investors, enhancing financial stability, and accelerating domestic savings. It is clearly evidenced that as financial intermediaries insurance companies kept direct and indirect contribution in the economic growth and development of the Kingdom of Saudi Arabia while the country is under serious pressure to eradicate the protection and restriction on the local market and struggle attain twofold objectives of survival and free trade as liberalization.
Due to WTO agreement, KSA has lost its sovereignty for economic policy setup, rather than considering the local market attributes and demand, it has to endorse the deregulation and liberalization (D&L) in the regulation and practice related to trade and commerce and the government has to provide open access to the foreign companies without protecting the local companies.
At the implication of compulsory health insurance, the most remarkable impact on the citizens is that they have habituated to transform their lifestyle with the health protection and formulating savings by providing premium of compulsory healthcare insurance that evidenced with 34% growth in the real premium accounted SR 9 billion in 2008.
Citizens, especially expatriates get assurance that their employers are taking care for their medical facilities, their treatment facilities may not unaddressed although they are not allowed to go to the public sector hospitals, at the same time, people also get enhanced opportunity to switch his job due to the increased job opportunities (SAMA 2010). The Colliers International (2012) pointed out that the increasing demand for among the increasing citizens has dramatically increased the private sector, the number private, quasi government and public sector hospitals are demonstrated in the following figure while the population reached at 26 million with 2.2% growth rate
Impact of Compulsory Medical Insurance on Governmental Budget
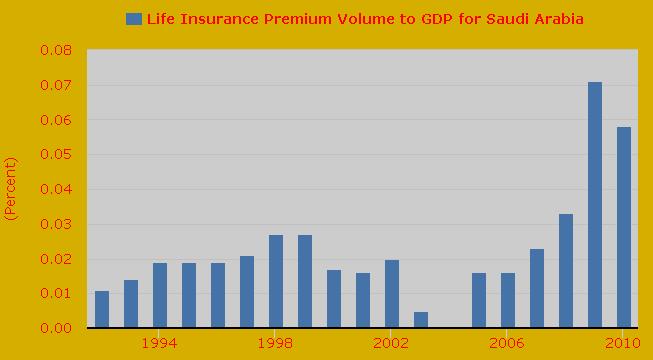
By using World Bank data and Sigma reports, the Federal Reserve Bank (2014) pointed out that compulsory medical insurance in KSA has evidenced a Ratio of premium volume to the direct GDP was 0.011 in 1992, 0.014 in 1993, 0.019 in 1994, 0.019 in 1995, 0.019 in 1996, 0.021 in 1997, 0.027 in 1998, and 0.027 in 1999. In the preceding years the contribution of medical insurance to the GDP has accounted as value 0.017 in 2000, 0.016 in 2001, 0.020 in 2002, 0.005 in 2003, 0.016 in 2005, 0.016 in 2006, 0.023 in 2007, 0.033 in 2008, 0.071 in 2009, 0.058 in 2010, this data has presented in the following graph.
Above data illustrated that contribution of compulsory medical insurance to the GDP of KSA is less then 1% to the of the GDP, but WHO (2005) presented that the governmental spending for public health was 8,597 thousand in 1990, 7,364 thousand in 1995, 11,939 thousand in 2000 and 14,756 thousand in 2004. The public health expenditure presented here was 6% of the GDP in 1990, 4.9% of the GDP in 1995, 7.6% of the GDP in 2000 and 6.4% in the respective years; thus, it is clearly evidenced that the privatisation public health in KSA and its consequential medical insurance has not yet enough contributed to the governmental budget and spending.
Compulsory Medical Insurance in other Countries
The Telegraph (2009) reported that the mandatory health insurance has turned into a trendy exploring the area of insurance business by introducing penal health insurance regulation for the expatriates in order to bypass the attributes of welfare state to provide fully fund the stipulation of healthcare service in the public sector. The World Bank (2008) that the compulsory health insurance that put into practise in different developing countries are very limited to the overall population while people urge for universal coverage for the healthcare service; thus, it is time to unify the healthcare service that could contribute to the overall economy although the cost consequences of such coverage related to resources.
In 2009, UAE planned to introduce mandatory health insurance for the expatriates working in the country, but due to global financial crisis this initiative was failed; thus, the country left this program for further study and implication while other GCC countries have already introduced this category of insurance. The United Kingdom has introduced mandatory health insurance for the expatriates working in the country and they urged that their implication of such insurance were correct, Australia, France, Holland, Spain and Abu Dhabi, has introduced mandatory health insurance in most recent years, but some of them implicated such insurance for al population.
Private Medical Insurance Globally
According to OECD (2011), private medical insurance today has very big responsibility all around the globe: governments of countries like Australia, Belgium, Canada, Denmark, France, Germany, Greece, Italy, Japan, Korea, Mexico, Netherlands, New Zealand, Norway, Poland, Spain, Sweden, Switzerland, Turkey, the United Kingdom, and United States frequently gaze to private medical insurance as a route to address medical scheme disputes.
Private medical insurance has changed the point of view of many nations, for instance, governments of these countries (mostly member states of Organization for Economic Cooperation and Development, OECD) deem to improve the function of private medical insurances so that they act as a substitute basis of medical funding and a mode to augment the aptitude of the entire scheme. In addition, the governments of these OECD countries also look forward to endorse private medical insurance as a utensil to advance extra medical course of action targets, which, for instance comprise augmented personal accountability; on the other hand, strategy creators at certain nations look upon to private medical insurance as a solution to their medical reporting schemes (OECD 2011).
Although private medical insurance symbolizes little portion of entire medical backing throughout New Zealand, Australia, Belgium, Canada, Denmark, France, Germany, Greece, Italy, Japan, Korea, Mexico, Netherlands, Norway, Poland, Spain, Sweden, Switzerland, Turkey, United Kingdom, and United States, it has major function in medical sponsorship at certain nations and entertains no less than thirty percent of the population of OECD region.
Private medical insurance has an assortment of functions, extending from basic treatment for specific inhabitant factions to supporting responsibility for public schemes; moreover, private medical insurance lifts people from definite disputes that mark the diverse responsibilities it have; however, policy makers need to intrude to tackle market breakdowns to guarantee private medical insurance admittance for high risk classes (OECD 2011).
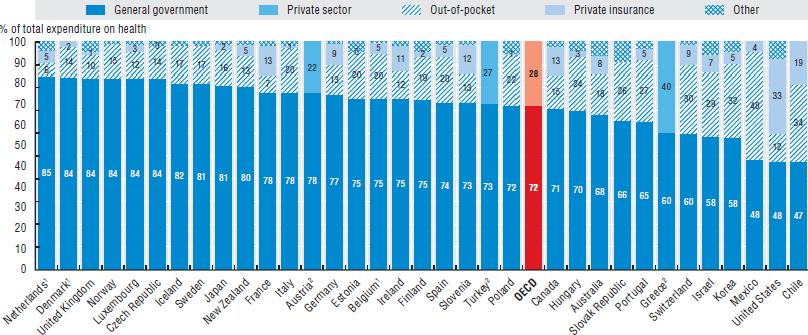
The following chart shows the medical expenditure by their source of medical funding in several member countries of Organization for Economic Cooperation and Development; it consists of a comparison of public spending on medical sector, private medical insurance, other private funds, as well as ‘out of pocket payments’ in those countries. This shows that even though public spending on medical sector is much higher than private medical insurance, and private medical insurance is quite lower than out of pocket payments as well, private medical insurance is increasing gradually and especially in the United States, it has been almost equal to public spending on medical sector:
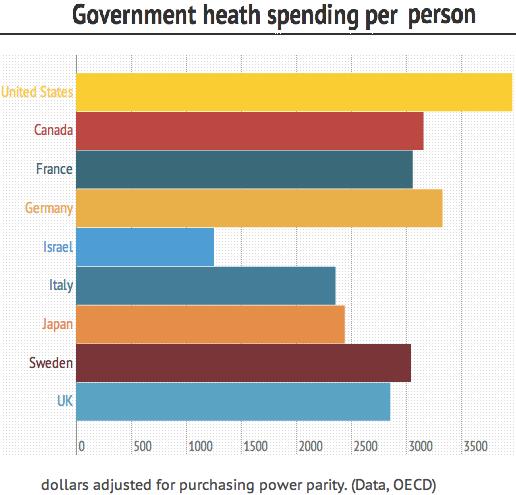
It is very important to state that the following chart shows the public medical expenditure per capita in OECD member states, which includes Germany, France, Israel, Canada, Japan, Italy, United States, Sweden, and the United Kingdom. It indicates that the public medical expenditure per capita is the highest in the United States, and second highest in Germany; in addition Canada is in the third position and Swenden and France is in the fourth; however, in most of the countries, this has not been substantial in comparison to other services (Klein 2013):
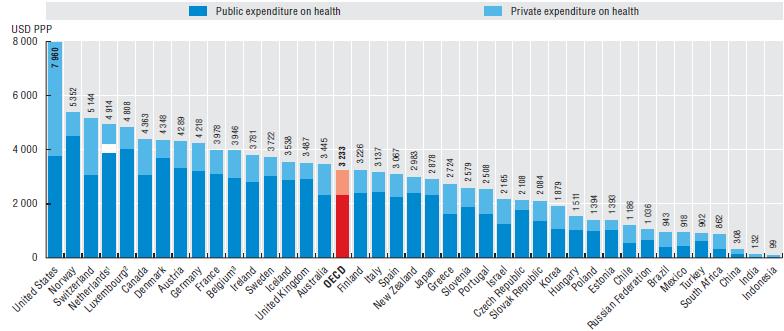
The following chart shows the total health care expenditure, which includes both public and private medical insurance as a percentage of the gross domestic product in the United States, Switzerland, Denmark, Ireland, Canada, Austria, Australia, Germany, France, Finland, Italy, New Zealand, Spain, the United Kingdom, Mexico, Poland, India, China, Turkey, Russia, Sweden, and so on. It is clear from the figure that the total health care expenditure, which includes both public and private medical insurance, is the highest in case of the United States, and second highest in case of Norway:
Benefits of medical insurance
It is important to note that numerous advantages of medical insurance are present in the market, for which people are persuaded to engage with it; for example, medical insurance liberates people from the panic and load of monetarily mounting medical fees as well as guarding them against the monetary jolt of an unforeseen health situation. In addition, it is also very much necessary to consider the fact that such kind of insurance not only saves cash of individuals, but also offers people better tranquillity of mind when they think of the probable penalties of any alarming health situations; most importantly, this coolness of mind can occur mostly in case of private medical insurances.
This is due to the reason that even if the most awful thing happens to an individual, the treatment would be as fast as possible, and people will easily feel the difference between the swiftness and easiness of services that the private medical insurances offer and the hassles that the public sector offers on the contrary. On the other hand, private medical insurances will also offer people the desire treatment in the most uncomplicated way; for example, people will not face problems associated with long rows; in addition, people will also have the opportunity to have a preference so that they can select their desired specialist and decide where they would like get the treatment.
If people wish, they can get the privacy during the whole treatment process, as they would not have to be anxious regarding staying at mixed gender area; this benefit will however depend on the policy that has been chosen; although it has to be admitted that one of the most vital benefit that will ensue is the unlimited visiting time. A high level of competition in the medical insurance market would mean that rival insurance firms would compete between each other to provide the best service possible; this will result in offering a very much skilled set of professionals dealing with individual’s health problems; several insurers would possess a panel that deals exclusively with a precise category of illness.
It is very much important to note that the most vital benefit this will have is the stability in treatment, as most people can expect to be checked by the same medical professionals during the entire period of the healing process; as a result, people will not have to explain and re-explain their physical problems to new set of doctors. There is no doubt that getting a medical insurance will offer an individual the chance to preserve and perk up their wellbeing through receiving an inexpensive means to go to the general practitioners, who would give reasonably priced recommendations regarding the medicines that are required; in addition, a number of schemes are supple so that people can tailor them accordingly.
All it means is that this will be very much affordable for average income earning families, who would be able to get the specialist treatment without spending much on procedural complexities; on the other hand, this will also eradicate the services from the package that has no need for an individual. It is a crucial factor to consider that when someone will turn out to be gravely sick or wounded, the medical scheme would include urgent situation handling system and a number of free surgeries as well; this indeed is a very important feature, as always people will not have cash in hand to deal with emergency costs of risky surgeries.
Suitable Balance between Public & Private Investment for Health Sector
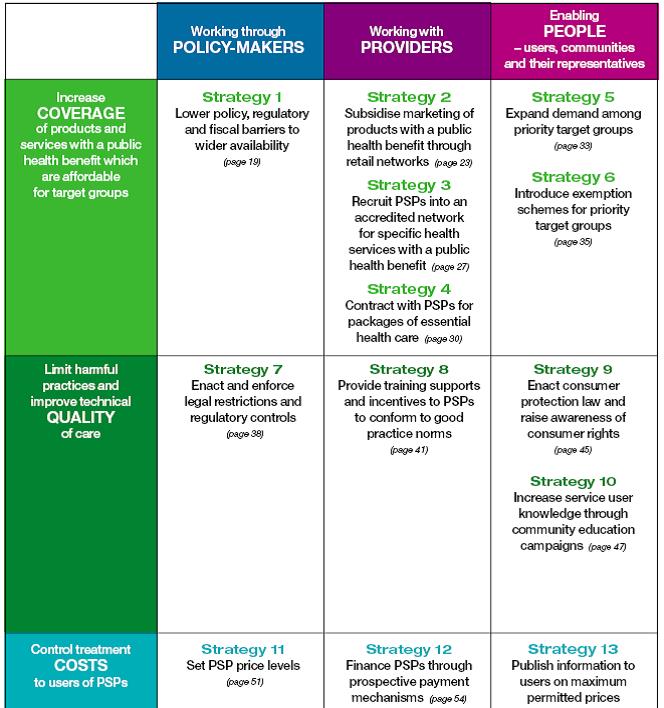
People first rely on private sector providers to diagnosis and treatment; however, poor people visit private clinics, but they have to switch off due to lack off resources and they receive ineffective treatment of serious diseases in most of the cases (Smith, Brugha & Zwi 2013). As a result, the researchers seem that suitable balance between public & private investment for health sector can enhance health care system of any place to ensure universal access and improved quality of care with the public-private mix of financing (Smith, Brugha & Zwi 2013); however, the following figure shows the policies for balancing with private sector providers:
Smith, Brugha & Zwi (2013) stated that international institutions promote private investment in health sector to improve performance.
Global Evidences of Health Sector Privatisation
In the era of globalisation, health plans in developing nations is influenced by the international institutions, such as, WTO, WHO, IMF and so on; in addition, developing nations are under severe pressure than ever to liberalize health care sector through privatise public sector services (Tellegen & Wemos 2012). According to the report of Tellegen & Wemos (2012), privatisation of public health care sector brings negative impact to the poor and vulnerable citizens of the developing countries, as they do not get basic health care services at present; in addition, the poor people received services at low cost, but now they have to pay more for ordinary services.
At the same time, the survey report identified that in Kenya, private hospitals discharge patients if they fail to afford further treatment and engage them in work to pay dues; moreover, in Nigeria, Thailand, and South Africa, hospitals management showed more interest on profit maximisation due to the adverse impact on privatisation (Tellegen & Wemos 2012). At the same time, Berer (2011) stated that privatisation has positive influence on the people to ensure quality service and standards of care, but most of the time poor people deprive from fundamental health care services due to lake of money; however, he further addressed that-
- The public sector has also turn into too costly for low income people to take service;
- Ill health is a foremost reason of indebtedness among the poor;
- No effective regulation to monitor private sectors for which it would be possible to ask higher charges for the services;
- Increase numbers of foreign patients while people of rural areas will be deprived from health care services (Berer 2011);
On the other hand, Albreht (2014) privatization in health care is the political agenda to the leaders of the developed countries; however, it has both positive and negative impact on the people and entire health care system and key issues include:
- Privatization plays vital role to satisfy the people while public service is poorly managed
- It creates a threat to equity and accessibility of medical facility due to increase cost for treatment;
- it develops parallel health care system, ensures quality of care, and good governance in this sector (Albreht 2014)
German Model of Health service
Clarke & Bidgood (2013) and Stiftung (2012) stated that health care system of German is well-known globally as good quality care; according to the provision Federal law, all the people have to obtain health insurance by using the facilities of the public-private partnership; therefore, about 85% people need to buy highly regulated, non-profit insurance GKV. At the same time, citizens of this country have to purchase insurance if net income €50,000 per year; about 10% buy private insurance and they pay in accordance with the income (Müller, Schmidt & Glazinski 2013; Clarke & Bidgood 2013; and Stiftung 2012).
On the other hand, the government of this nation strictly regulates sickness funds, which fall into six major groups; however, GKV mainly connected with industries (Müller, Schmidt & Glazinski 2013; Clarke & Bidgood 2013; and Stiftung 2012). However, the people of this country believes in solidarity for which the government takes responsibility to assure universal access through public health care services; however, the government will not establish public sector monopoly, but develop the concept of social partnership (Müller, Schmidt & Glazinski 2013; Clarke & Bidgood 2013; and Stiftung 2012).
GKV covers both short-term and long-term care through separate insurance scheme; here, it is significant to mention that long-term care is mandatory for the entire population considering individual care needs; however, the cost will vary person to person, for instance, people with no children have to pay more (Müller, Schmidt & Glazinski 2013; Clarke & Bidgood 2013; and Stiftung 2012). However, the government of this country had taken many controversial initiatives for the health sector, but they ensure a sound and stable health care system in national level; however, the following figure shows health care expenditures from 1992 to 2009:
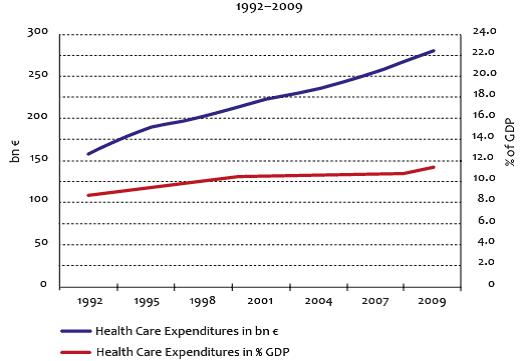
As the expenditures for health care services had increased dramatically, the government concentrates on the private health insurance to cover certain statutory health insurance co-payments; however, SHI includes Preventive and Physician services, Rehabilitation – Mental health care, Dental services, Prescription drugs (Müller, Schmidt & Glazinski 2013; Clarke & Bidgood 2013; and Stiftung 2012). However, the model of health service of this country controls through three types of organisations, such as, publicly owned, non-profit private and for-profit private; however, the next table gives more detail in this regard:
Table 1: Hospitals in Germany. Source: Müller, Schmidt & Glazinski (2013)
The above table demonstrates that the dependency on publicly owned has decreased by 14.5% within 18 years; however, Müller, Schmidt & Glazinski (2013) stated that this trend has shifted due to financial problems in the municipalities, focus more on the concept of privatisations. On the other hand, the share of non-profit sector remained stable, but numbers of private hospitals had increased significantly due to the adverse effect of privatisation (Müller, Schmidt & Glazinski 2013; Clarke & Bidgood 2013; and Roeder & Labrie 2012). The government has reformed considering economic conditions, social status of the people, and many other financial indicators; however, the existing model of German Health care service is a perfect model for the citizens though only 30% hospitals are state owned.
American Model of Health Care Service
According to the report of Irvine (2013), the health sector of this nation constructed with both public and private funding; however, both private and public sectors ensure high quality services though there is few dilemmas; therefore, the government had enacted the Affordable Care Act 2010 to reduce these dilemmas and begin universal medical care system in this country.
The main objective of this act was to change present healthcare system; however, it focused on many areas, such as, development of Medicare’s long-term financial outlook as there were about 42 million Medicare beneficiaries, implement Medicaid programme in order to offer healthcare service for the poor people, offer of subsidies to low-income people and so on (Irvine 2013). In addition, this act is expected to cost US$1.1 trillion within the next ten years, to cover 32 million currently uninsured people, to raise total coverage to 94 percent of the inhabitants by the next five years, to give people rebates along with discounts on brand name drugs and to reduce inefficiencies in Medicare Advantage (Irvine 2013).
At the same time, the reform health care system will give the opportunity to more 16 million individuals to be qualified for Medicaid (Irvine 2013; and O’Neill & O’Neill 2014); however, other important factors are new provisions include through insurance reforms, and insurance exchanges. However, the next table includes key features of different health care programme in the USA:
Table 2: Different health care programme in the USA. Source: Self generated
Summary
From the above discussion, it can be said that the international institutes created huge pressure on the government of the member states to ensure open access to the foreign companies in the national health care sectors for which these institutes suggest to concentrate on the privatization of public health care sectors. The content of this literature illustrates the effects of privatization on the citizens, and governments in health sectors of both developed and developing countries; in addition, this paper compares the position of public health care of KSA with the USA and Germany.
At the same time, it addressed that the government of KSA has already changes rules and regulation in order to develop the concept of privatisation of public health care sector; however, the people of this country will get better services due to increase of competition in this sector, but the overall cost for treatment will increase as well. The impact of privatisation of health insurance sector over the citizens of the Kingdom of Saudi Arabia after the execution of the Health Insurance Act (1999) has remained optimistic; increasing competition among the companies that offer the insurance policies are in fact benefiting people with superior and high quality services. In addition, there exist several benefits of medical insurance through the Saudi Arabia from an overall point of view.
Reference List
Ahmad, J 2011, ‘Impact of Reforms on Insurance Industry of Saudi Arabia’, Interdisciplinary Journal of Research in Business, vol. 1, Web.
Ahmed, M 2013, Kingdom of Saudi Arabia: Healthcare Overview.
Albreht, T 2014, Privatization processes in health care in Europe—a move in the right direction, a ‘trendy’ option, or a step back.
Almalki, M, Fitzgerald, G & Clark, M 2011, ‘Health care system in Saudi Arabia: an overview’, Eastern Mediterranean Health Journal, vol. 17, no. 10.
Bagaresh, A 2013, Accession of Kingdom of Saudi Arabia’s To World Trade Organization and Its Benefits, Web.
Berer, M 2011, Privatisation in health systems in developing countries: what’s in a name? Web.
CHIC 2009, Implementing Regulations of the Cooperative Health Insurance Law in the Kingdom of Saudi Arabia (Amended), Web.
Clarke, E & Bidgood, E 2013, Healthcare Systems: Germany, Web.
Colliers International 2012, Kingdom of Saudi Arabia Healthcare Overview, Web.
Eljelly, A. M. A 2009, ‘Ownership and Firm Performance: The Experience of Saudi Arabia’s Emerging Economy’, International Business & Economics Research Journal, vol. 8, No. 8, Web.
Federal Reserve Bank 2014, Life Insurance Premium Volume to GDP for Saudi Arabia.
Irvine, B 2013, Healthcare Systems: USA, Web.
Klein, E 2013, Two charts that should be in every health-care discussion, Web.
Ministry of Economy and Planning 2010, The ninth development plan 2010–2014 for Saudi Arabia, Web.
Müller, P, Schmidt, B & Glazinski, B 2013, Understanding the German Health Care System, Web.
OECD 2011, Health at a Glance 2011.
O’Neill, J & O’Neill, D. M 2014, Comparing the U.S. and Canadian Health Care Systems.
Roeder, F. C & Labrie, Y 2012, Privatization can bring efficiency gains to public hospitals.
SAMA 2010, The Saudi Insurance Market Report 2010, Web.
Smith, E, Brugha, R & Zwi, A 2013, Working with Private Sector Providers for Better Health, Web.
Stiftung, R. B 2012, Structure of the German Health Care System.
Tellegen, N & Wemos, D 2012, Access to health care for all – Risks of trade in health services and the impact of privatisation, Web.
The Telegraph 2009, Compulsory Health Insurance Has Become ‘Fashionable’.
The World Bank 2008, Governing Mandatory Health Insurance Learning from Experience, Web.
WHO 2005, Health Systems Profile- Saudi Arabia: Health Care Finance And Expenditure, Web.
WHO 2013, Country Cooperation Strategy for WHO and Saudi Arabia 2012–2016.