Patient Information
Jane Doe was a female 35-year old patient who presented to the clinic for the first time as the records indicated. She was white, stood at 172 cm in height, and weighed 57 kilograms. Jane initially came to the clinic with her husband and was assigned to a physician who analyzed her case before referring her to the lab for several tests. She complained that she was constantly tired, felt weakness in her knees plus elbows, and pain and swelling of her knees and elbows. Jane also complained of pain in the muscles around her knees. The pain was incredibly intense whenever she tried to conduct any physical activity such as running or walking.
History of Present Illness
The patient, upon inquiry, informed the doctor that she had noticed knee and elbow pains during her routine evening runs two months ago. She had dismissed the pain as fatigue and taken a rest from her runs before resuming and the case being the same. She worriedly informed her husband about it, who brought her home aspirin for the pain. The drugs helped lessen the pain during her runs but did not eliminate it entirely. The two of them agreed to visit the clinic for an examination and professional help.
Past Medical History
The patient had no prior hospitalizations or illnesses and no known chronic diseases but reported to have suffered from pneumonia two years ago. Records from her previous physician showed that she had been infected with Mycoplasma pneumonia. The doctor had treated her pneumonia with several drugs, and she had eventually achieved full recovery.
Family History
On family history, she explained that her mother’s side of the family had this condition prevalent. Her late grandmother had experienced joint pains when she was around 60 years. Her knees could not support her during her late years, and she relied on a wheelchair until her death. Her mother had experienced slight joint pains when she was around 55 years but had sought treatment early, and her progression was not as fast as her grandmother’s. Some of her aunties had experienced the same issue, and she was worried that the same would happen to her.
Social History
Jane smoked cigarettes leisurely but was not a chronic smoker. She lived with her husband in their home with their dog. She did not have any children as they had decided not to have any with her husband. They lived in a posh estate within the city, and both drank alcohol as they had a bar in their house.
Physical Examination
Upon a physical examination, Jane was found to have the following values. Her body temperature was 36o C (standard 37o C), her blood pressure was 127/83 mmHg (normal 120/80 mmHg). Her resting pulse at the time was 70 beats per minute (normal 60-100 beats per minute), while her respiration was 15 breaths per minute (normal 12-16 breaths per minute) (Johns Hopkins Medicine). The doctor examined Jane’s joints and discovered some swelling and redness. The doctor tested joint function and range of motion by asking the patient to move around and move her joints to various degrees. The examination revealed pain on flexion and extension of knee and elbow joints. Jane also had limited muscle strength as she couldn’t easily lift things. Upon touching her elbows and knees, her joints were warm and tender.
Lab Data
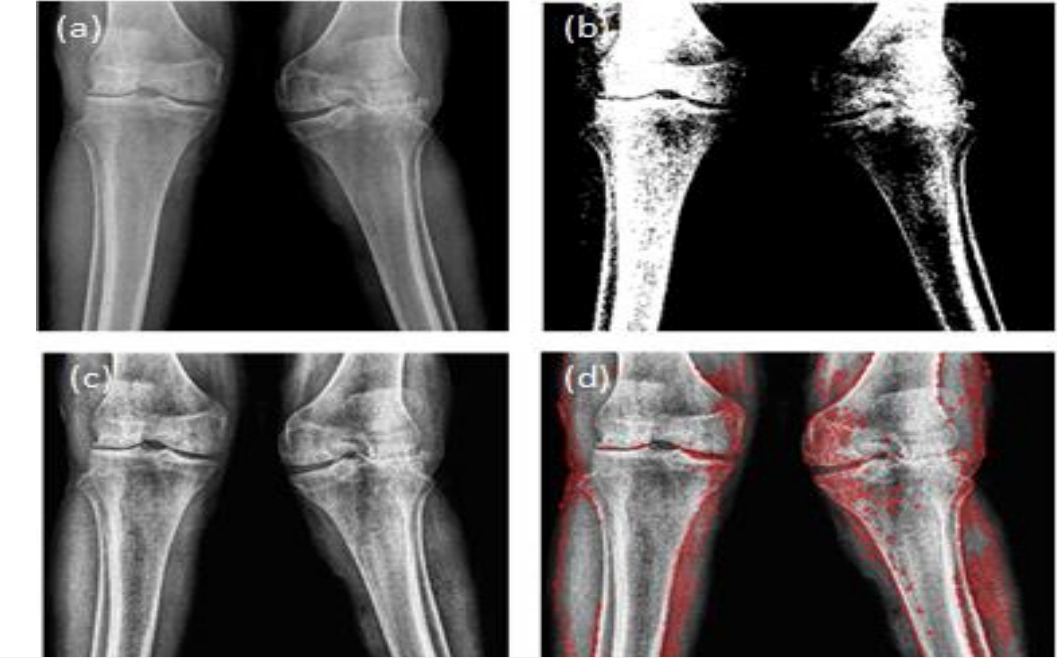
The doctor suspected rheumatoid arthritis and sent her for several tests in the laboratory for confirmation. The doctor sent her for a knee X-ray and several blood tests. The X-ray result was similar to the one provided in the appendix as figure 1, and it is affirmative for rheumatoid arthritis (Snekhalatha et al.). The joint had bony erosions, loss of articular cartilage, and narrowing of joint space. Blood tests include a rheumatoid factor test that checks for a protein called rheumatoid factor that is associated with rheumatoid arthritis, and the patient had 18 IU/ml (normal is <16 IU/ml) (Daien et al.). Anti-CCP test looks for an antibody associated with rheumatoid arthritis, and the patient value was 24 Units (normal is <20 Units). An erythrocyte sedimentation rate (ESR) test was also recommended and checks for whether inflammation is present. Patient had a higher ESR value of 35mm/hr (normal is 0-30mm/hr).
A C-reactive protein test was also ordered and helped confirm whether inflammation is present. C-reactive protein is produced by the liver whenever there is inflammation in the body. Rheumatoid arthritis leads to widespread inflammation within the joints and other body organs when it spreads, and this protein is therefore produced in sufficient amounts during this condition. The patient had a value of 1.7 for her C-reactive protein, while the normal value is 1.0. The final test ordered by the doctor was a complete blood count. The complete blood count would indicate the severity of the disease and whether any other complications had arisen in the blood. The complete blood count revealed that the white blood cell count was 11.4 (normal 3.8-10.8), red blood cell count was 3.4 (normal 3.8-5.1), hemoglobin 9.8 (normal 11.7-15.5), platelets 160 (normal 140-400)
Final Recommended Treatment
Rheumatoid arthritis is not a curable treatment, but its progression can be slowed, and the symptoms managed. Various medical procedures can be used to ensure that the condition does not progress to the chronic stages that immobilize the patient quickly (Mohan 843–844). Some of the symptoms that should be managed for rheumatoid arthritis patients include pain. Pain ensures in rheumatoid arthritis patients when they engage in activities such as walking or running. Manual labor that involves the flexion and extension of arms is also painful and may interfere with a person’s ability to perform at their job. Movement may be hampered and render one in need of support such as wheelchairs for movement (Abbas et al. 818–821). Slowing the progression of the damage to the joints is the available medical treatment procedure for this disease. Slowing the progression of the disease also ensures it does not affect other body organs outside the joints. This disease can affect the heart and respiratory system if it progresses without sufficient management.
Corticosteroids are crucial in rheumatoid arthritis as they reduce inflammation and pain. The favorable corticosteroids for Jane are prednisone and hydrocortisone. These corticosteroids should be injected directly into her joints to alleviate the pain and reduce inflammation, generally slowing the progression of the disease (Wei et al.). Other immunosuppressants such as methotrexate lessen the production of the rheumatoid antibodies responsible for the condition, ensuring progression is slowed down (Friedman and Cronstein). These should also be injected into the most affected joints. Tumor necrotic factor (TNF) antagonists such as infliximab are crucial in inhibiting TNF activity (Quistrebert et al.). TNF causes synovial cells to secrete proteases that destroy hyaline cartilage in the joints, hence rheumatoid arthritis. In addition to medical treatment, Jane should indulge in low-impact exercises to increase the range of mobility of her joints, such as gentle yoga (Metsios and Kitas). She should ensure she gets enough sleep and rest to reduce fatigue, inflammation, and pain. Applying heat with warm showers and hot compresses can reduce stiffness. Applying cold with cold compresses can reduce inflammation and pain and also reduce muscle spasms.
Works Cited
Abbas, Abul, et al. Robbins Basic Pathology. Elsevier.com, 10th ed., Philadelphia, Elsevier, 2017, pp. 818–821, Web.
Daien, Claire, et al. “Update of French society for rheumatology recommendations for managing rheumatoid arthritis.” Joint Bone Spine, vol. 86, no. 2, Mar. 2019, pp. 135–150.
Friedman, Benjamin, and Bruce Cronstein. “Methotrexate mechanism in treatment of rheumatoid arthritis.” Joint Bone Spine, vol. 86, no. 3, Aug. 2018, pp. 301–307.
Johns Hopkins Medicine. “Vital signs (body temperature, pulse rate, respiration rate, blood pressure).” Johns Hopkins Medicine Health Library, 2019. Web.
Metsios, George S., and George D. Kitas. “Physical activity, exercise and rheumatoid arthritis: effectiveness, mechanisms and implementation.” Best Practice & Research Clinical Rheumatology, vol. 32, 2018, pp. 669–682, Web.
Mohan, Harsh. Textbook of Pathology. Medicos Times, 8th ed., Daryaganj, Jaypee Brothers Medical Publishers, 2018, pp. 843–844.
Quistrebert, Jocelyn, et al. “Incidence and risk factors for adalimumab and infliximab anti-drug antibodies in rheumatoid arthritis: A European retrospective multicohort analysis.” Seminars in Arthritis and Rheumatism, vol. 48, 2019, pp. 967–975,
Snekhalatha, U, et al. “Automated segmentation of knee thermal imaging and X-Ray in evaluation of rheumatoid arthritis.” International Journal of Engineering & Technology, vol. 7, no. 2.8, 2018, pp. 326–330.
Wei, Bo, et al. “Corticosterone suppresses IL-1β-induced MPGE2 expression through regulation of the 11β-HSD1 bioactivity of synovial fibroblasts in vitro.” Experimental and Therapeutic Medicine, vol. 13, no. 5, 2017, pp. 2161–2168.
Appendix