Introduction
Quincy is the 8th largest city in Massachusetts, USA, and is located in Norfolk County. As of 2009, Quincy town had a population of 91, 073 persons (U.S. Census Bureau, 2009). The city is located to the Northern side of Boston and the Western side of Milton with the Neponset River marking its borders with the two states. To the south, it is separated by the Fore River which marks the border with Weymouth. To the East, Quincy shares a border with Hull (Wead, 2005, p. 59).
Within Quincy’s borders, the Hangman, Moon, Nut and Racoon Islands are all found and according to the United States Government; the total area covered by the town, including the islands is 26.89 square miles (Forbes Hill, USGS, 2010). Of this total surface area, 16.8 square miles is dry land while 10.1 square miles is covered with water. Comprehensively, about 37% of Quincy is covered in water (MassGIS, 2008). Although a great part of the town is urban, a good portion of Quincy is under reserved land. This land is largely uninhabited and maintained by the state. A great portion of the Southwestern part of the city is also uninhabited.
Initially, Quincy was part of Doechester around 1630 but it was annexed by Boston four years later and then renamed, Braintree (Lodge, 1902, p. 7). The area was largely under English colonialists who settled there to practice farming because of the area’s favorable agricultural climate. In 1972, during the time of the American Revolution, Quincy obtained its own identity by having its own name, John Quincy. By 1888, the town had fully grown and developed economically to attain a city status (Adams, 1891, p. 3). Initially, the city was known for its rich iron business, stone cutting, shipbuilding and aviation but today, its economy is much more diverse (Jabaily, 2007).
Quincy has a fair climate but it is prehistorically associated with tornados (Quincyma, 2010). The climate is generally conducive for farming, with moderate rains and potentially sunny seasons witnessed throughout summer. However, the place generally experiences cold weather for most of the year (Boston Harbor Association, 2010). Housing is adequate for most Quincy residents with proper sanitation services provided by the municipality.
The municipality is therefore the major stakeholder in the provision of basic social, amenities like water and sanitation services. The municipality also forms the government because Quincy is largely categorized as a municipality and headed by a mayor. The mayor is therefore the main appointing authority for all city departments including the health department and his role towards the proper functioning of the town cannot be underestimated (City of Quincy, 2009, p. 1).
This study will develop a community assessment program based on the city with the aim of creating a care plan for tackling the issue of child obesity in the town. The above statistics are important in assessing the geography and governance of the city to determine the feasibility of healthcare services in the region. With regards to the demographic characteristics of Quincy, the city currently has approximately more than 88,000 households with a population density of approximately 5 people per square kilometer (U.S. Census Bureau, 2009).
Current estimates project that there are approximately more than 40,000 housing units at an average density of 2,388.8 square miles. In terms of racial segregation, approximately 80% of the population is white, 2% African American, 0.2% Native American, 15% Asian, and 0.03% Pacific Islanders while the rest are from other races (U.S. Census Bureau, 2009). Of the total population, Hispanics and Latinos constitute approximately 2% but of this population group, about 34% are of Irish origin, 13% of Italian origin and about 6% of English origin. Of the entire population described above, about 80% of the people speak English, 10% speak Chinese dialects, 2% speak Cantonese, I.5% speak Vietnamese dialects and the rest speak Italian as their primary language (U.S. Census Bureau, 2009).
Of the total households in Quincy, statistics show that about 21% have children considered as minors (under the age of 18) in their custody; close to 40% of the households have competed families (with the father and mother cohabiting together); about 10% of households are characterized by a female living alone (without a male companion); about 47% of households are not family setups and 37% of them are made up of individuals living by themselves. Also, approximately 14% of the total households have an adult above the age of 65 living alone (United States Census Bureau, 2003, p. 26). The average size of a Quincy household is estimated at two people but the average family is estimated at 3 people (U.S. Census Bureau, 2009).
In urban centers, the number of teenagers (those below the age of 18) is estimated at slightly less than 20% while the rest of the population groups constituted 8% for people between the age of 18 and 24, 1% for people between the age of 25- 44 and 22% for people between the age of 45 and 64. Finally, about 135 of the population were aged above 65 years. The median age for city inhabitants is 38 while the ratio of men to women is: for every 100 women there are 92 males (for adults) while for those aged below 18; for every 100 females, there are 87 males (U.S. Census Bureau, 2009).
The average income for a typical Quincy household is approximately $48,000 but the median income is safely above $60,000 (U.S. Census Bureau, 2009). However, males earn higher than their female counterparts because their median income is projected at $41,000 while that of females is projected at $35,000. The income per capita for the entire city is projected at $28,000 but approximately 5% to 7% of the total population is feared to be living below the poverty line (U.S. Census Bureau, 2009). In terms of age group classification, about 10% of the population aged below 18 years is living below the poverty line while 7% of adults aged above 65 are living under the same circumstances (U.S. Census Bureau, 2009).
These statistics are important in determining the lifestyle patterns of the population because some of the most severe forms of obesity are determined by the lifestyle patterns of the population. Nonetheless, the income levels of the population are important in assessing the capability of the population to afford healthcare. The higher the income level the more capable the population is in affording healthcare.
Childhood Obesity
Quincy has had a relatively comparable child mortality rate with the entire country. However, the major causes of child mortality in the city are factors such as birth defects, cancer, heart complications, pneumonia, flu and injuries caused by accidents or carelessness of the parents. Other common factors contributing to child mortality include drowning, fires, falls and suffocation (Greve, 2007, p. 3).
Nonetheless, Quincy has reported increased cases of childhood obesity which is feared to worsen the community’s health in coming years. Quincy has therefore in the recent past been grappling with the problem of childhood obesity with most initiatives aimed at containing the health risk. The Harvard Pilgrim Health care foundation and other similar organizations have consequently launched health programs to keep young children healthy in light of changing lifestyle patterns in Massachusetts and indeed the entire country.
It is bad enough that obese children go through psychological trauma and rejection from their friends and society but they also serve the risk of increased health complications such as liver problems, sleep apnea, type-two diabetes, high blood pressure and cardiovascular complications. Obese children have also been identified to run high risks of hypertension, digestive disorders while in their advanced ages (as adults), they are likely to be less economically empowered and more likely to die earlier than their thinner counterparts (Greve, 2007, p. 4).
Incorporating the statistics Massachusetts health department provides; there seems to be a big childhood obesity issue not only in Massachusetts but indeed the entire state. For instance, in Quincy, low to middle-income households contribute up to a third of childhood obesity cases in the city. A youth health survey was undertaken in 2007 also points out that approximately 20% of children in Middle school run high risks of becoming overweight but at the same time, more than 10% of the total population in middle school are already overweight (Greve, 2007).
Obese high school students in Quincy are projected to be around 15% of the total high school-going population. These statistics have tremendously increased and in fact almost doubled because statistics projected that about 7% of the high school population in 1999 were obese while 11% of the same population group were also obese in 2007 (Greve, 2007). These statistics have been affirmed at the Quincy public school for children in the first, fourth, seventh and tenth grade between the period of the year 2005 and 2008 through BMI testing (Greve, 2007). More accurate data between the periods of 2007 and 2008 are provided below:
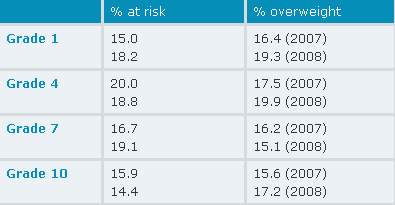
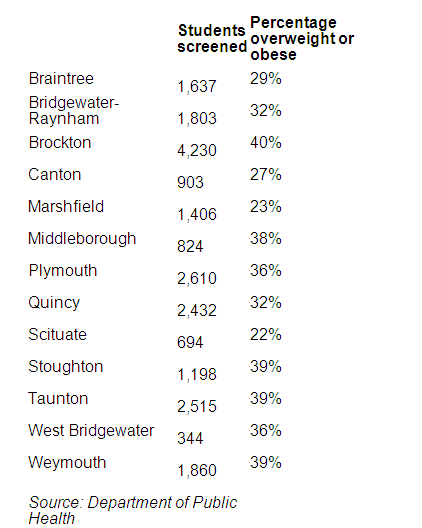
From the above comparison, it is evidently clear that Quincy records obese rates comparable to national statistics. Lambert (2010) also notes that one in every five children in the town is currently obese. This fact is derived from a study to gauge obesity prevalence in Quincy schools based on the body mass index and the weight of the children. It was later confirmed that Scituate schools had among the lowest rates of childhood obesity after Arlington and four other communities although obesity rates in the town were still at an all-time high with Marshfield having obese rates slightly above 23% and Weymouth also having obese rates slightly above 38%. Lambert (2010) still identifies that other schools in the South Shore district had obese rates in the following manner “Stoughton, 38.7; Plymouth, 35.5; Quincy, 32.2; Braintree, 29.4; and Canton, 27.3” (p. 7). Overall, these statistics project that in every sample of 110,000 students, approximately 34% were obese. These statistics can be further broken down as follows:
These figures have prompted many initiatives within schools to minimize calorie intake among students. Vending machines for example have been painted with many health messages that discourage against unhealthy foods. However, obesity is not the only health concern for the youth in the city because there have been increased cases of drug abuse and diabetes which have also greatly impacted on the community.
These lifestyle diseases have been noted to be on the increase because there is a reduced level of activity among Quincy teenagers and most of them do not observe a good diet that is supposed to boost their health. In addition, many teenagers do not exercise at all. Comprehensively, Quincy seems to be suffering from an acute problem of lifestyle diseases that need to be curbed before it turns out into a future catastrophe.
Community Planning
Childhood obesity is considered a bad health risk and has stood out in the past few years not only in Quincy but in America in general. It now stands as one of the biggest forms of health risk in the present generation. Child obesity is not difficult to notice as a medical condition though its treatment and management is a hard task. Nationally, obese conditions brought about by a lack of proper dieting are estimated to cause approximately 300,000 deaths (Greve, 2007, p. 10).
The treatment and management of this condition are also very expensive, with statistics estimating that childhood obesity potentially costs society up to $100 billion (American Academy of Child Adolescent Psychiatry, 2009, p. 6). The situation is much worse for children because they are more likely to fall victim to obesity than adults. At the same time, they are likely to live longer with the condition, thereby complicating their lives even further.
Normally, childhood obesity is variable because not all weight gain is considered as obesity. However, when a child’s weight is 10% more than the recommended weight for the child’s body type and height, the said person is obese (American Academy of Child Adolescent Psychiatry, 2009, p. 6). Obesity is often noted to begin in the early years of childhood, between the ages of 5-6 and is known to progress to later stages of adolescence. Statistics projecting adult obesity as a result of childhood obesity are also not encouraging because current data suggest that obese children who are between the ages of 10-18 have an 80% likelihood of becoming obese adults (American Academy of Child Adolescent Psychiatry, 2009, p. 6).
Treatment and management of obese patients is a difficult task because it is not easy to determine the real cause of obesity. However, obesity is caused by a number of known factors such as genetics, biological trends, cultural habits and poor lifestyle patterns. However, in literal terms, obesity comes from a low burnout of calories than is presently consumed. Despite statistics pointing out that medical disorders can cause obesity, the likelihood of this happening is very rare because less than one percent of obese cases arising from medical disorders have been reported (American Academy of Child Adolescent Psychiatry, 2009, p. 7).
Nonetheless, when obesity occurs, patients need to seek proper checkup by a physician to asses the possibility of treatment or physical management. In most instances, the treatment and management of childhood obesity is not difficult because it may wholly or partially involve increasing physical activities to increase calorie burn out; unless the condition is physical. A permanent solution can only be realized when there is an absolute sense of commitment from the patient. The role of a nurse is therefore to enable patients achieve a high sense of motivation and also assist them get the best treatment incase the condition is physical and cannot be solved through regular exercising or be minimized through a lifestyle change.
The reason why many teens slide back into weight gain is because of the fact that obesity is a lifelong matter and when most patients lose weight, they often assume they have achieved their goal and go back into their old lifestyle habits. Obese children therefore need to enjoy their new lifestyle patterns that enabled them to lose weight in the first place and not perceive it as a short-term measure or as a type of punishment. In nursing and management of obese children, it is important that nurses focus on the strengths of the patients as opposed to the issue at hand (weight).
There is a huge emphasis on parents and other relevant authorities to reduce the availability of carbohydrates, carbonated drinks, sweets and other foods that have high calorie content away from children. In fact, parents should be encouraged to celebrate occasions like birthday parties by cooking healthy foods that will improve the health of their children as opposed to cooking food substances such as cakes (Lambert, 2010). Due to the complexities of instilling a healthy diet on children, it is important that this approach be implemented slowly and with the input of all stakeholders.
Due to the fact that children who experience an obesity problem already suffer emotional problems, it is important that a comprehensive plan be devised to contain he comprehensive effects of obesity. Such a plan will have to outline specific short-term goals, incorporate physical exercising, diet modification, behavior change and family participation. These are the grounds through which this study will develop a care plan for childhood obesity in Quincy. Formulating short-term goals will be a primary strategy, incorporating physical exercises and diet modification will be secondary strategies while advocating for a behavior change and seeking family participation will be tertiary strategies.
Community Health Care Plan
This community care plan will be multifaceted because it touches on all the critical factors that contribute to child obesity. More comprehensively, it acknowledges the input of all stakeholders in containing the issue. In a detailed manner, this community healthcare plan will identify seven sectors that impact on fundamental aspects of childhood obesity and will further go ahead to identify two areas of action that need prompt attention (in every sector). Childhood obesity being a complex issue, many programs can cover some milestone in eradicating the problem altogether. However, this community health care program will provide a framework through which many partners can work together and compare their progress with each other (NuPAC, 2009).
State and Local community level
First, with the collaboration of the Quincy mayor and other local authorities, Quincy should launch a workable community program whereby paths and walkways need to be built along major residential and town streets to promote physical exercising. This approach should however also be done in collaboration with school boards, such that important matters of concern such as security issues, biking, and policies regarding food in public places are streamlined such that there are no conflicts on policy matters. Sample policy statements should thereafter be provided before such a measure is implemented and later, member organizations will be identified to lead such initiatives.
Secondly, the local authorities should expand the access people have to public facilities. This will improve household health at a local level including nutrition and physical activities so that parents are sensitized on the healthiest ways to reduce childhood obesity. This initiative should also be led at the forefront by voluntary advocates and a sample language template should also be provided to outline how the initiative is expected to be handled.
Family Level
First, strategies to promote the consumption of healthy food among families should be encouraged through neighborhood workgroup programs for families during mealtimes. Families should therefore be sensitized to take on the most nutritional foods for children aged below five years and also on the need to eat meals in a family set up, whenever it may be workable for the children. The importance of fruits and vegetables in family meals should also be emphasized.
This should also be done through sharing cultural foods that are acceptable and nutritional for children. Also this program should be done in the context of making family meals fun for children to avoid instances where children feel enslaved to such programs. Efforts by responsible parents and community advocates should also be brought to fore because they will act as role models for the children in adopting appropriate nutritional lifestyles.
Secondly families should be sensitized on the importance of undertaking family activities to increase the playtime with their children, hence increasing the level of physical activity for the children. Brainstorming should therefore be done to give families new ideas on activities they could undertake with their children such as taking family walks (both in their residential areas and at school). The brainstorming should also be done in collaboration with school authorities and local authorities (for access to parks and recreational facilities because Quincy is well known for its breathtaking nature sites).
Neighborhoods where such activities can be supported should also be made known to the parents and school authorities so that such activities can be undertaken in such localities. Youth volunteers should also be consulted so that they can coordinate such efforts to increase physical activity among children. Also comprehensively, parent advocates need to be encouraged to take part in such activities because they will stress the importance of regular physical activities to children and indeed act as role models to other parents so that they uphold an active family life with their children. Another strategy on the same would be to create more opportunities where parents can increase their participation or lend their support towards programs that encourage physical activity for their children.
Heath care Service Providers and Insurance Companies
First, health care providers should launch preventive standards of care which foster physical activity among children in a way that is appropriate for their age groups and in a manner that conforms to the conventional culture of Quincy inhabitants. Health care providers should also promote various preventive measures established by concerned bodies at a local or national level, such as the American Medical Association’s Expert Committee.
Health care providers should provide collaborative programs with other health care facilities on critical areas such as the training of nurses to promote and implement preventive care programs. This should be done in collaboration with child organizations operating in Quincy. Later on, a follow up should be undertaken to ensure high standards of care and ongoing preventive programs, are being properly undertaken.
Secondly, health care providers should refer patients and their families to appropriate resource programs available at Quincy which can compliment their preventive efforts. Again, a list of resources that can supplement their efforts to prevent childhood obesity and treat it should be compiled and availed to the parents. A list of resources should also be compiled by other children organizational groups even for ailments that arise out of obesity such as diabetes or high blood pressure and availed to parents. These lists should however be first deliberated with health care planners, professionals, parent advocates and other partners of the community to ensure parents and their children are referred to resource centers that are appropriate for their problems. Insurance should thereafter come in to improve payment methods where interested parties can conveniently pay for these services without much difficulty.
Schools
The strategy outlined below will majorly incorporate the input of the Quincy department of education and more so, the participation of the mayor in facilitating the department’s efforts. The department of education should therefore launch a dietary program in the context of nutritional education to encourage parents and teachers alike to promote healthy food and beverage policies that reduce child obesity in the long run. The practice should be able to meet or at times exceed the mandate given to the school by state or federal agencies. More importantly, this practice will instill a healthy eating habit among schoolchildren to avoid their overall intake of unhealthy foods.
Unhealthy food and beverage advertising should therefore be limited in all schools within Quincy. The promotion and distribution of only healthy foods should therefore be encouraged at all costs so that children have limited access to foods that only promote their health. This practice should be implemented through the advancement of healthy foods as an alternative to unhealthy foods which children are already used to. Class celebrations and all other activities that go on within the school should also be graced by serving strictly healthy foods. This should be implemented as far as club events, classroom celebrations, and even in events such as fundraising where parents, teachers and children will be required to observe a healthy diet as well.
A school breakfast program should also be promoted and implemented in schools which will have a significant number of children willing to enroll in the program. Promotion of the importance of nutritional foods should also be undertaken together with the above initiatives by painting educational messages on school locker rooms, hallways and such public places. The importance of eating nutritional foods should also be promoted as part of the physical education program where students will be encouraged to eat healthy foods as part of the physical education after program. Also the input of parents and student leaders can never be ignored because they will help in the promotion of a good and healthy environment for the children.
Alternatively, through relevant authorities, extra physical educational policies that compliment state and federal policies or supersede them should be implemented to improve children’s physical health and fitness standards. Later, teachers should be oriented on the best method of implementing such a program. With regard to physical classes, these programs should be emphasized as much as academic content is.
A standard should thereafter be established regarding what is strenuous, impractical, vigorous or moderate so that children can take part in certain types of activities that correctly suit them. With an increase in physical activities and more emphasis on physical education achieved, more public-private partnership needs to be fostered so that children can use existing educational facilities more freely. This will increase the quality and quantity of children’s physical activity throughput their time in and out of school.
Employers and Work Sites
Employers in work sites should be sensitized on the importance of serving healthy foods during important events where children are allowed to attend. A guideline should therefore be provided to highlight the type of healthy foods that can be convenient for both adults and children to enjoy. In the same manner, a sample outline should be provided to interested parties so they have a rough idea of the best foods to serve in meetings and events. This initiative is aimed at setting the right precedent for children because they learn best from their parents and older folks.
Apart from diets and food measures, more physical activity should be encouraged at work sites. This can be done by encouraging people to use the staircase more often and using walk paths, pedometers, lockers, showers and such like facilities especially during important meetings and events (which will act as an example to young children coming up). This initiative should also be undertaken through the provision of guidelines that are aimed at improving physical activity in the long run. The most common methods of physical activity such as stairway use should be most encouraged because children easily pick up on such elements.
Materials that support such initiatives should be visible in most public places within the work place context because children are frequenters of such zones, especially when they visit their parents or in such like circumstances. Such measures should not be downplayed because research has shown that children best pick their poor lifestyle habits from older people. Moreover, such an initiative is majorly aimed at instilling a responsible culture not only to children but parents as well.
Food and Beverage Sectors
The suppliers of food and beverage in Quincy especially need to be brought on board in implementing overall childhood obesity reduction programs because there is a need to post calorie information when packaging different types of foods. However, this type of commitment requires effective legislation and so the local authority should also be on board. On another front, restaurants should be required to post nutritional information on their menu boards. At the same time, they should also be sensitized to develop healthy foods that are most appropriate for children.
In addition, the preparation of quality and healthy foods should be done in a variety of ways so that parents have a wide choice to choose the best food for their children. At the same time, the general community should be willing to assist in identifying sources for healthy foods within neighborhoods so that the expansion of consumption of healthy foods such as fruits and vegetables is encouraged.
Entertainment and Sporting Events
Children are common frequenters of sports events and children entertainment funfairs. With this fact in mind, it is important to promote the consumption of healthy foods during such events because children are easily inclined to consume “junk” foods in such kind of events. Policy guidelines should therefore be implemented in forcing event organizers to avail healthy foods in such events.
Partnership should also be fostered with agencies willing to supply healthy foods to funfairs and negotiations need to be done with event organizers and venue owners to ensure such an initiative is a success. Such negotiations should especially be fostered in movie theatres where children are common frequenters because healthy snacks need to be availed in such places. Lastly, the community should consider investing in public facilities to promote physical activities through the availability of funds to support public places which ensure healthy foods are availed (Scribd, 2010).
Conclusion
Quincy is strategically located to implement most of the strategies identified in this study. Its huge endowment of recreational facilities and strategic governance structure can effectively see through the recommendations in this study. Considering the city suffers some of the worst rates of child obesity in the entire state, it is important that Quincy take a proactive approach in reducing child obesity in the area.
This study acknowledges the importance of curbing child obesity through the input of many stakeholders. Obesity being a multifaceted problem, it is important that strategies are developed to encompass all the relevant areas that need to be explored. In this manner, this study specifically identifies the input of the state and local authorities, parents, school boards and the general community at large in dealing with child obesity at Quincy.
However, a bulk of the responsibility rests on the community and parents at large because it is the future of the community which is at stake. If childhood obesity is left unchecked, Quincy may have a disaster in future because childhood obesity is on an increasing scale and immediate measures need to be employed to curb the problem. If the above policies are effectively implemented, such a problem may be eradicated in the coming future but key in its success is the unrelenting commitment of all the stakeholders involved.
References
Adams, C. (1891). History of Braintree, Massachusetts (1639-1708): The North Precinct of Braintree (1708-1792) and the Town Of Quincy (1792-1889). Cambridge, MA: Riverside Press.
American Academy of Child Adolescent Psychiatry. (2009). Obesity in Children and Teens. Web.
Boston Harbor Association. (2010). Beaches. Web.
City of Quincy. (2009). City of Quincy Departments. Web.
Forbes Hill, USGS. (2010). Geographic Names Information Service: 612914. Web.
Greve, F. (2007). Death Rate for US Children Falls. Web.
Jabaily, R. (2007). Coping with Economic Change: Quincy, Massachusetts. Boston: Federal Reserve Bank of Boston.
Lambert, L. (2010). Scituate Schools Get High Health Marks In Obesity Study. Web.
Lodge, H. (1902). Boston. New York: Longmans, Green, and Co.
MassGIS. (2008). Protected and Recreational Open Space Data. Web.
NuPAC. (2009). Orange County Obesity Prevention Plan: A Plan of Action 2009. Web.
Quincyma. (2010). About Quincy Beaches. Web.
Scribd. (2010). Family Nursing Care Plan. Web.
United States Census Bureau. (2003). Census 2000: Massachusetts: 2000 Population and Housing Unit Counts PHC-3-23. Web.
U.S. Census Bureau. (2009). Table 5. Annual Estimates of the Resident Population for Minor Civil Divisions in Massachusetts, Listed Alphabetically Within County. Web.
Wead, D. (2005). The Raising Of a President: The Mothers and Fathers of Our Nation’s Leaders. New York: Atria Books.