Early diagnosing is important for the patient population with symptoms that can be consistent with acute coronary syndrome (ACS) because the wrong diagnosis and premature discharge can have tragic consequences. The monitoring of the undifferentiated population with acute chest pain in the traditional hospital setting is ineffective, costly, and time-consuming.
On the one hand, the physicians cannot discharge the patients before making sure that these symptoms are not consistent with cardiac diseases, on the other hand, the prolonged monitoring procedures mean the ineffective use of the hospital resources. The organization of Chest Pain Units (CPUs) in the traditional hospital setting is the innovative method of monitoring, diagnosing, and treatment of patients with undifferentiated acute chest pain.
Though the establishment of the CPU requires expenses on buying the equipment, creating the conditions for the clients, and training the nursing staff, the early diagnosing and development of effective intervention programs for the patients with cardiac diseases allows distributing the hospital resources more reasonably. Blomkalns and Gibler (2005) emphasized the economical benefits of the CPUs along with their practical value: “admissions for ultimately diagnosed ‘noncardiac’ chest pain cost our society billions of dollars annually. The CPU has allowed physicians to condense a hospital admission into a 6- to 12-hour evaluation, risk stratification, and observation period” (p. 418). Corresponding to both economical and practical priorities of the health care system, the organization of CPUs is beneficial for the patients and the medical institution in general.
The organization of CPUs allows early diagnosis of the patients with acute chest pain, effective treatment of those whose symptoms are consistent with ACS, and discharge of the rest, increasing the patients’ satisfaction with the quality of the services and decreasing the physicians’ risks of misdiagnosing.
The undifferentiated patient population with acute chest pain presupposes diagnostic difficulties for the physicians and high risks of misdiagnosing. The traditional approach to testing and monitoring these patients in the hospital setting is expensive and time-consuming while the premature discharge of patients whose symptoms are consistent with the acute coronary syndrome (ACS) may have tragic consequences. These circumstances gave rise to the debates and searches for alternative methods of diagnosing this patient population.
Chest Pain Units (CPUs) are the innovative systems of monitoring and treatment of patients with acute chest pain whose symptoms can be consistent with cardiac diseases. These units are organized as a part of the traditional hospital setting and have all the necessary equipment for conducting all the necessary tests and evaluating all the measurement results as well as the specially-trained nursing personnel.
The establishment of the CPUs requires solving the problems of dedicating space to the unit, buying the equipment, creating additional comforts for the patients and visitors, and training the staff. For this reason, the effectiveness of the CPU and its appropriateness for the particular medical institution should be evaluated critically before the beginning of the reorganization process. The evidence-based practice (EBP) approach to decision-making in health care presupposes conducting thorough research and reviewing the literature before proceeding to the implementation of the reorganization plan.
The critical analysis of the latest studies concerning the advantages and disadvantages of organization of the CPUs as the alternative method of monitoring and diagnosing the undifferentiated patient population with acute chest pain is important for evaluating the effectiveness of the method and its impact on the intervention output, patients’ satisfaction and working conditions of the nursing staff.
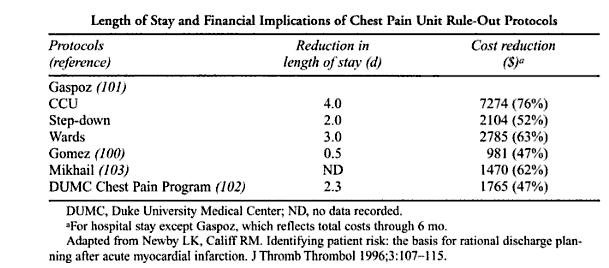
Appendix 1 (Adapted from Cannon, 2003, p. 201)
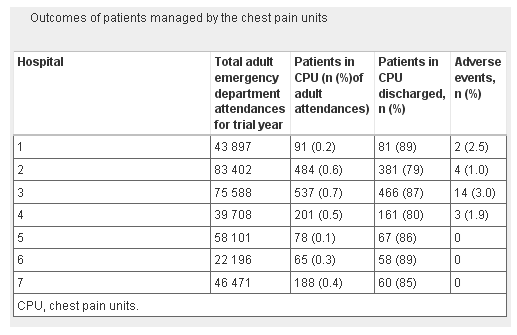
Appendix 2 (Adapted from Cross & Goodacre, 2010)
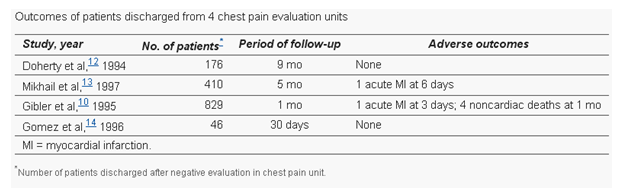
Appendix 3 (Adapted from Quin, 2000)
References
Arnold, J., Goodacre, S., & Morris, F. (2007). Structure, process, and outcomes of chest pain units established in the ESCAPE Trial. Emergency Medicine Journal, 24(7): 462-466.
Blomkalns, A. & Gibler, W. (2005). Chest pain unit concept: Rationale and diagnostic strategies. Cardiology Clinics, 23: 411-421. Web.
Cannon, C. (ed.) (2003). Management of acute coronary syndromes. Totowa, NJ: Humana Press.
Cross, E. & Goodacre, S. (2010). Patient satisfaction with chest pain unit care: Findings from the Effectiveness and Safety of Chest Pain Assessment to Prevent Emergency Admissions (ESCAPE) cluster randomized trial. Emergency Medicine Journal, 27: 774-778.
Goodacre, S. et al. (2005). Which diagnostic tests are most useful in a chest pain unit protocol? BMC Emergency Medicine, 5 (6). Web.
Quin, G. (2000). Chest pain evaluation units. Western Journal of Medicine, 173(6): 403-407.