Gender-Related Factors
Mental health characteristics differ among males and females from adolescence onwards. During development, gender dissimilarities have been discovered in various factors. Men are more likely than women to suffer from schizophrenia as they develop the illness at a younger age than women. Females appear to have stronger premorbid and sociability than males. According to Sommer et al. (2020), men with schizophrenia and first-episode psychotic symptoms are more likely than women to consume addictive substances. In terms of disease progression, women have higher recovery rates and fewer relapses. Nonetheless, the proportion appears to be equal since men with schizophrenia are more likely to die by suicide or fatality than women.
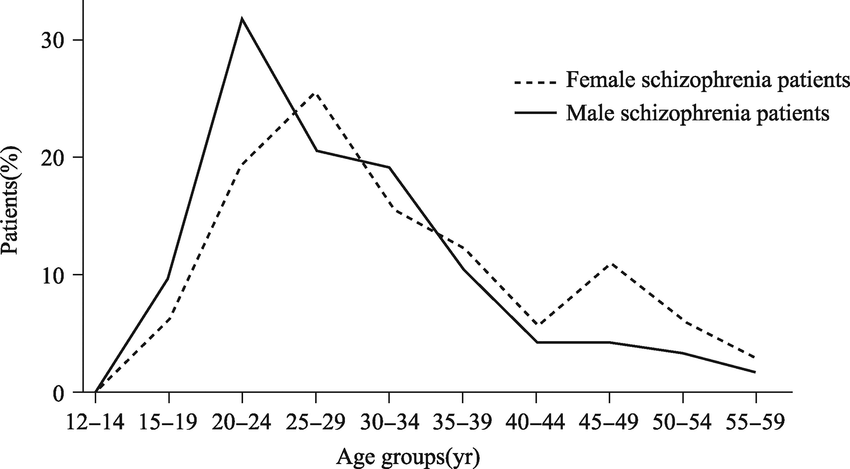
Schizophrenia strikes swiftly and unexpectedly, which leads to remission intervals. Most people experience it gradually, with minor warning signals and a progressive reduction in function. Li et al. (2018) say that men’s symptoms of schizophrenia usually appear in their early to mid-20s, whereas women’s symptoms appear in their late 20s, as indicated in figure 1 below. Patients with schizophrenia suffer from cognitive deficits, notably in the areas of memory span, delayed recollection, and language. While the sex disparities disorder between male and female schizophrenia patients needs to be investigated further, research has found that male schizophrenic patients have more severe brain abnormalities in direct and disrupted memory than female patients.
Sex variations in brain structure and functions have been linked to a female’s rapid and delayed cognition preference. Since the symptoms of schizophrenia in females differ from those in men, they are more likely to be misdiagnosed, lowering their chances of a positive outcome. Women have a higher probability than men of suffering from mood disorders, emotional problems, eating disorders, Stress, traumatic disorder, social phobia, and self-harm. Females tend to develop difficulties before or during their delivery, such as low birth weight, preterm labor, and a shortage of oxygen (asphyxia) during childbirth (Chen et al., 2018). These factors may have a minor impact on brain functioning.
Sex & symptoms
Schizophrenia has varied effects on men’s and women’s sexual life. These effects could be due to variances in the start of schizophrenia at different ages. Women living with schizophrenia have better emotional results, have longer relationships, and have more children than males with schizophrenia. However, interpersonal and social limitations hinder the formation of permanent sexual relations in both genders. Women are more likely than men to acquire schizophrenia in the future, according to Gogos et al. (2019), potentially due to the impact of sex hormones on the brain. Riecher-Rössler et al. (2018) investigated the sexual activity and views among chronic inpatients with schizophrenia, a factor that has contributed to hospitalization and made sexuality challenging, and found that the majority of the female patients were still interested in sex. About half of them wanted to get pregnant, but many were unclear about their shortcomings as parents.
Sexual dysfunctions are an essential element in treatment outcomes, which are impacted by antipsychotic health risks and other outcome variables like well-being. Other factors are involved, as sexual dysfunction can be noted in undiagnosed schizophrenia patients: One of the consequences in men is decreased libido due to unpleasant sensations (Stusiński & Lew-Starowicz, 2018). Human neural growth is affected by the steroids and hormones linked with sex differentiation in fetal growth. According to Stusiński and Lew-Starowicz (2018), there is proof that these hormonal changes have repercussions for sex variations in brain abnormalities reported in adults with schizophrenia. Men diagnosed with schizophrenia had more serious brain damage than women based on magnetic resonance imaging studies. Stusiński and Lew-Starowicz (2018) pointed out that sexual behavior in people with schizophrenia differs comparatively and quantitatively from that of individuals without the condition. Although people with schizophrenia have lower total sexual activity, they are more likely to participate in autoerotic behavior.
Symptoms of schizophrenia manifest themselves in various ways as the condition progresses. Alert signals of schizophrenia are sometimes missed until puberty. Social disengagement, despair, difficulties in concentration, aggression, insomnia, poor personal hygiene, or unreasonable views are indicators. Men with schizophrenia tend to have more side effects and clinical traits than women, especially social disengagement, substance addiction, and dulled or incongruent results. Women with schizophrenia are likely to experience mood swings, depression, and affective symptoms. While various biological, societal, and lifestyle variables may contribute to these gender differences, the importance of gonadal steroid hormones has become increasingly apparent (Riecher-Rössler et al., 2018). Females undergo distinct endogenous changes in ovarian hormone levels throughout their lives, which influence the symptom pattern of central nervous system illnesses. However, men tend to lose joy or desire to live and retreat from society.
Estrogen defense
Schizophrenia is a varied mental condition that manifests differently in women than men, although not generally milder. The preventive role of estrogens has been related to differences between the sexes. A female sex hormone, estrogen, significantly impacts the brain’s chemical processes. Menopausal females’ estrogen levels have decreased, linked to a rise in schizophrenia symptoms. It has long been known that when the estrogen rate is low, women are more sensitive to antipsychotic medicines and respond negatively to them. As a result of the research was done by Veerman et al. (2017), evidence supporting the use of estrogen as a treatment demonstrated that it relieves patients’ positive symptoms. Therefore, this hormone’s incorporation into regular therapies may help men with schizophrenia.
Estrogens control key pathophysiological processes in schizophrenia, such as dopamine activation, membrane potential, and stress response (Veerman et al., 2017). The well-known “estrogen hypothesis,” which claims estrogen protects against schizophrenia, is the most popular explanation of these sex differences. According to (Veerman et al., 2017), estrogen influences dopamine systems. Estrogen appears to function as a hindrance to dopamine receptors in investigations of schizophrenia. As a result, estrogen may help avoid the rise in dopamine seen in schizophrenia patients. This backs up the theory that estrogen works as a defense, explaining why the occurrence of schizophrenia in women peaks in their late forties. Estrogen levels diminish in women, leading to dopamine levels to rise, resulting in psychosis.
Adjunctive estrogen therapy can help women with schizophrenia have better results. According to Veerman et al.’s (2017) research, women with schizophrenia need to be provided with estrogen doses in their mid-twenties and forties when estrogen levels are low. This might improve the efficacy of antipsychotic medicines and aid women with schizophrenia in leading regular lives without experiencing schizophrenia episodes in their forties. Concerns about feminization have influenced men’s decisions about estrogen therapy. Lab tests employing estrogen to treat prostate cancer, bone loss, and even violence in men with dementia have shown estrogen to be a safe and effective treatment (Veerman et al., 2017). However, the data imply that more research into the therapeutic potential of adjunctive estradiol in men with schizophrenia is needed. Estrogen may thus be a critical element in treating psychotic symptoms in men who have schizophrenia.
Epidemiologic Patterns
Schizophrenia affects people throughout the world, but significant differences have been observed regarding the disease epidemiology between men and women. The global prevalence of Schizophrenia (i.e., the proportion of incidents in a group at any one time) is approaching 1% (Petkari et al., 2017). With the high increase in social stressors and anxiety, the prevalence rates have been rising in all genders. According to Petkari et al. (2017), the annual incidence (number of new cases) is approximately 1.5 per 10,000 persons. The age of onset is among the primary factors in epidemiologic studies.
Notably, the onset is affected by social, psychological, and emotional conditions. In both male and female schizophrenic patients, adolescence is the most common age of onset (Petkari et al., 2017). In this case, adolescence is viewed as beginning from thirteen years and progressing to twenty-one years. Across both genders, cases involving infancy and late life (beyond 45 years) are uncommon. Males are diagnosed with the condition at a somewhat higher rate than women, in a ratio of 1.4:1 (Petkari et al., 2017). Although the onset lies within the youth age, women are diagnosed later than men, with the latter showing symptoms as early as 18 years (Petkari et al., 2017). This is significant because it denotes how gender exposes individuals to the disease at different rates and in various proportions in time.
In women, two different phases are evident in regard to a schizophrenia diagnosis. According to Petkari et al. (2017), psychosis diagnosis in women occurs from 25 years, with a second peak occurring around their menopause years. It is worth noting that although schizophrenia diagnosis in women occurs later in life, they have a higher life expectancy of the condition. This means they are more likely to suffer from the disease for longer compared to men.
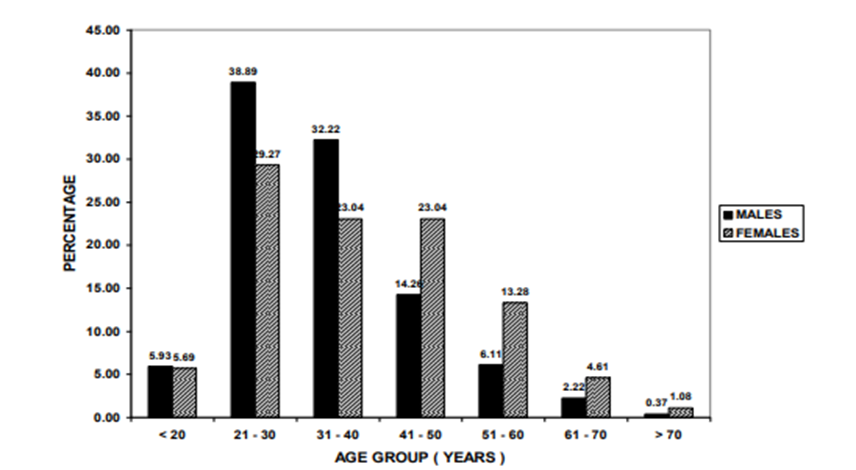
In a study conducted in an Indian hospital, clear-cut epidemiologic differences were observed, confirming the theoretical knowledge existing on the subject. As shown in fig. 2 below, the age cohort 21-30 years had the highest number of both genders, with 210 patients (38.89 percent) being males and 108 patients (29.27 percent) being females (Mathew et al., 2020). In addition to onset, the prevalence of Schizophrenia in old age was investigated. Minimum patients (n=6) were over the age of 70, with two patients (0.37 percent) being men and four (1.08%) being females (Mathew et al., 2020). The variation of epidemiologic patterns with age is crucial for better health management practices.
The age of onset and prolonged schizophrenia symptoms has been a focus of research among researchers. The relationship between gender and epidemiology, as suggested by Petkari et al. (2017), was confirmed in this study, where males represented a higher proportion than females in the categories below 20 years to 40 years. Mathew et al.’s (2020) study showed that females were more than males in the age groups above 40 years, proving their longer life expectancy of the condition. However, these results depend on other gender factors such as social roles.
Symptomatology
The set of symptom characteristics and their significance differ between men and women diagnosed with Schizophrenia. According to Li et al. (2017), men with the condition tend to have more symptoms of mental illness and clinical traits than women, especially in terms of social disengagement, substance addiction, and incongruent feelings. The severity of these symptoms depends on age and other psychological factors. Since they tend to be more disengaged, men may experience may show negative characteristics for more extended periods than women. Comparatively, women with Schizophrenia have higher mood disturbances, depressive symptoms, and affective symptoms than men (Seeman, 2019). Surprisingly, such sex-specific characteristics in male individuals with Schizophrenia were also seen in people at high risk for the illness.
The type of symptoms is closely linked to the age of onset. For example, women with delayed Schizophrenia may have fewer psychotic symptoms and more positive characteristics, such as persecutory delusions and sensory hallucinations, according to Seeman (2019). Patients with Schizophrenia suffer from cognitive deficits, notably in the areas of immediate memory, delayed memory, and language. While the sex disparities between male and female patients with schizophrenia symptoms need to be investigated further, recent studies have found that male patients have more severe cognitive impairments in short-term and prolonged memory than their female counterparts (Li et al., 2017). However, these differences do not include language, spatial visualization, or attention indices. Sex variations in the structure of the brain and activities have been linked to a female’s preference for immediate and delayed memory. These differences are crucial because they inform the development of gender-specific treatments and therapy.
Gender Differences in Clinical Therapy
In recent years, gender-specific psychosis treatment options have been proposed. Gender differences may help doctors prescribe more appropriate and gender-based psychotherapeutic treatments, including drug dosage, adverse effects management, and medication adherence. According to Lange et al. (2017), female patients have a greater therapeutic response than male patients and require around half as many hospitalizations. Men with psychosis generally require higher antipsychotic drug dosages due to their increased liver enzymatic clearance (Lange et al., 2017). Male psychiatric patients also smoke more cigarettes and drink more coffee, both of which accelerate medication clearance by liver enzymes. Therefore clinicians have to use the appropriate gender-specific approaches to ensure that men and women receive the best schizophrenia treatment.
The age-gender association has also provided an explanation for the variation in therapeutic approaches for men and women. Postmenopausal women required antipsychotic doses more than younger women, which was linked to a decrease in endogenous estrogen levels (Li et al., 2017). Since hormones may interact with antipsychotic drugs, studies have shown that estrogen therapy, either alone or in combination with antipsychotics, results in speedier recovery in individuals of both genders with psychosis (Lange et al., 2017). The response to treatment options is partly related to the chemical composition of the drugs administered and their impacts on patients. Li et al. (2017) allude that since most antipsychotics have adverse reactions, studies have shown that women have more of such effects, including hyperprolactinemia, hypotension, excess body weight, and immunological proclivity enhancement.
Medication adherence differs significantly between the two genders, determining the additional steps that should be enforced to facilitate patient recovery. In Li et al.’s (2017) study, women had higher medication adherence and better treatment outcomes than men. Since men and women react differently to schizophrenia treatment, therapy for men may focus on managing substance abuse, establishing socio-occupational competence, and decreasing negative externalizing behaviors (Li et al., 2017). Comparatively, treatment for women may focus on reducing affective symptoms and alleviating comorbid anxiety and depression. In addition, since many women experience a later start of disease and larger socio-occupational losses, research has recommended that women’s therapy should focus on re-defining roles and strengthening relationships, whereas men must achieve these for the first time (Li et al., 2017). In summary, therapeutic approaches should be tailored to accommodate gender differences regarding medication adherence, adverse effects, and dosage requirements.
Social Perception of Illness
Men and women view Schizophrenia differently, impacting their response in terms of sociological interactions. According to Seeman (2019), men are less likely to accept the illness and seek medication. Although they show symptoms earlier than women, men withdraw from society rather than seek help from the community. In contrast, women tend to be more open, viewing Schizophrenia as a disorder that requires more engagement and relationships. Building on this information, Lange et al. (2017) argues that re-establishing social connections would be more helpful for women than men. Evidently, the association of psychosis with social factors and the development of viable solutions from the same determines how well individuals respond to the illness.
The causes of an illness have been deemed a social factor that significantly alters people’s perception of it, influencing their approaches to themselves and other patients. According to Belayneh et al. (2019), women are more likely to hold traditional beliefs about the causes of Schizophrenia than men. However, the difference in social views can be attributed to varying socio-cultural environments in which individuals live. The study by Belayneh et al. (2019) revealed that females were 1.7 times more likely than men to have traditional perceptions of the causes of Schizophrenia. In essence, depending on the sociocultural influences, women are more likely to develop social perceptions of Schizophrenia than men.
References
Belayneh, Z., Abebaw, D., Amare, T., Haile, K., & Abebe, Z. (2019). Perception regarding the causes of schizophrenia and associated factors among Feresbet district residents: A community-based study. BMC Public Health, 19(1), 1-7. Web.
Chen, L., Selvendra, A., Stewart, A., & Castle, D. (2018). Risk factors in early and late-onset schizophrenia. Comprehensive Psychiatry, 80, 155-162. Web.
Gogos, A., Ney, L. J., Seymour, N., Van Rheenen, T. E., & Felmingham, K. L. (2019). Sex differences in schizophrenia, bipolar disorder, and post‐traumatic stress disorder: Are gonadal hormones the link? British Journal of Pharmacology, 176(21), 4119-4135. Web.
Lange, B., Mueller, J. K., Leweke, F. M., & Bumb, J. M. (2017). How gender affects the pharmacotherapeutic approach to treating psychosis–A systematic review. Expert Opinion on Pharmacotherapy, 18(4), 351-362. Web.
Li, R., Ma, X., Wang, G., Yang, J., & Wang, C. (2017). Why sex differences in schizophrenia? Journal of Translational Neuroscience, 1(1), 37–42. Web.
Mathew, V. K., Sam, K. G., Samuel, B., & Das, A. K. (2020). Epidemiology of schizophrenia in an Indian hospital. Research Journal of Pharmacy and Technology, 13(1), 219-223. Web.
Petkari, E., Mayoral, F., & Moreno-Küstner, B. (2017). Gender matters in schizophrenia-spectrum disorders: Results from a healthcare user’s epidemiological study in Malaga, Spain. Comprehensive Psychiatry, 72, 136-143. Web.
Riecher-Rössler, A., Butler, S., & Kulkarni, J. (2018). Sex and gender differences in schizophrenic psychoses—A critical review. Archives of Women’s Mental Health, 21(6), 627-648. Web.
Seeman, M. V. (2019). Does gender influence the outcome in schizophrenia? Psychiatric Quarterly, 90(1), 173-184. Web.
Sommer, I. E., Tiihonen, J., van Mourik, A., Tanskanen, A., & Taipale, H. (2020). The clinical course of schizophrenia in women and men—A nation-wide cohort study. NPJ schizophrenia, 6(1), 1-7. Web.
Stusiński, J., & Lew-Starowicz, M. (2018). Gender dysphoria symptoms in schizophrenia. Psychiatria Polsca, 52(6), 1053-1062. Web.
Veerman, S. R., Schulte, P. F., & de Haan, L. (2017). Treatment for negative symptoms in schizophrenia: A comprehensive review. Drugs, 77(13), 1423-1459. Web.