What are the major motivation issues at play in the health care industry according to the major needs-based theories of motivation (Maslow’s need hierarchy theory, McClelland’s acquired needs and Deci & Ryan’s self-determination)? What motivation theory is more popular expectancy theory or Herzberg’s two-factor theory? Keep reading to find out!
Introduction: Role of Motivational Theories in Healthcare
Lack of a motivated workforce is one of the impediments to the achievement of the millennium development goals in the context of healthcare. This is due to a lack of motivation among health care workers and especially in low and middle-income generating countries leading to poor provision of healthcare. There is a loss of clinical staff and this further cripples the health care system, which is already fragile due to insufficient workforce (Dieleman & Harnmeijer, 2006).
The lack of motivation among the health workers is as a result of inability by the health service managers to meet the needs of these health workers. It is, therefore, necessary that health service managers develop the appropriate mechanisms to retain and motivate health care workers. Health service managers need to understand the various theories that govern the motivation of health workers to work to ensure their motivation and retention in the workplace (MHEN & VSO, 2011). This paper will discuss why it is essential that health service managers understand what motivates health worker by looking at their needs with the help of various motivational theories.
Motivational Theories in Healthcare: Discussion
According to Deci and Ryan (2000), motivation is the impetus drive to do something. There is sufficient evidence to support the fact that workers’ performance is highly dependent on the level of motivation by the workers (Garcia-Prado, 2005; Rowe, 2005; Marsden, French & Kubo, 2000; Vroom, 1970). Different theories have been put forth to argue out the fact that the motivation to work is governed by various needs, which if not satisfied de-motivate workers to indulge in productive work and efforts.
Motivational Theories: Maslow’s-Hierarchy of Needs Theory
Abraham Maslow proposed the Maslow’s-Hierarchy of needs theory that outlines five universal needs as the main motivating factors for people (Dolea & Adams, 2005; Zurn et al., 2005). One thing to note with Maslow’s hierarchy of needs is that a lower must be significantly fulfilled before moving on to the next higher need on the hierarchy. His hierarchy of needs theory ranks the needs based on their level of influence on human behaviour as indicated in the figure below (Maslow, 1954):
To start with, there are physiological needs, which are considered to be the lowest-level needs and include needs such as food and water. When these needs are not satisfied in a person’s life, a driving/motivating force is created and it seeks to achieve these needs. When a person is hungry, this person develops a felt need that gives rise to psychological and physical tensions, which can be realized by the person’s overt behaviour aiming to reduce such tensions that result from the need to eat. After the person gets something to eat, the hunger and the resulting tensions are reduced. This is applicable in the case of a health worker who has various physiological needs, which motivates the health worker to continuously provide health care to patients. This way, he/she would get paid after his/her services hence can meet his/her physiological needs (Benson & Dundis, 2003).
When a person’s physiological needs are satisfied, they move on to the next needs, which according to Maslow’s hierarchy of needs are the safety. Safety needs include needs for shelter and security. Safety and security needs entail the desire for “security, stability, dependency, protection, freedom from fear and anxiety, and a need for structure, order, and law” (Hughes et al., 2002). Safety and security needs by health workers translate into a need for employment security and as such will stop at nothing until they are assured for continued employment.
Health workers will, therefore, engage in high levels of effort and productivity so that they do not lose their jobs. Subsequently, social needs are next and entail the need for belongingness and love. In the workplace, health workers aim at satisfying their social needs through interacting with colleagues, superiors and subordinates. The ability to work with others in peace and establish good working relations motivates the workers to put all their efforts to work because peace and good working relations with other workers define good working conditions (Benson & Dundis, 2003).
Once social needs have been met, there is the need to satisfy workers’ ego and esteem. The workers seek to achieve “self-respect, self-esteem and esteem of others” as intrinsic components of the esteem need (Dieleman & Harnmeijer, 2006). Also, there is an external element of the esteem need and it entails the need for “reputation, prestige, status, fame, glory, dominance, recognition, attention, importance, and appreciation” (Zurn et al., 2005).
In this context, health service managers need to understand that how a health service manager manages and/or supervises the health workers greatly determines the health workers’ motivation about their ego and esteem needs. If managerial and/or supervisory roles are given to adept and qualified individuals then it is not difficult to motivate the health care workers. Highly qualified leaders and managers know how to lobby for resources to ensure that the health workers’ needs are addressed and met hence giving them the motivation they require (King & McInerney, 2006).
Good communications with a caring leader/manager is a great motivating factor for the health workers as they appreciate a leader or manager, who is ready to listen to their voices thus, the health workers feel obliged to work as per the desired expectations. As a health service manager, therefore, it is important to understand that health workers’ needs are paramount if quality health care outputs are to be obtained. A health service manager should always ensure that he/she is committed to the welfare of the health workers; this will motivate them to give their best since they are aware that their efforts are valued (Gray, 1991). Health service managers should understand the need to motivate health workers based by creating good relations with them to satisfy their social needs.
Self-actualization is the highest need according to Maslow’s hierarchy. Self-actualization entails the need for self-realization and continuous development. This is the point in time when a health worker seeks to become the best person they can be. It is facilitated by career opportunities that enable health workers to grow and develop professionally. Career opportunities are very vital to an employee since, one aims at climbing up the ladder of job promotion (Benson & Dundis, 2003). Therefore, health managers must develop strategies to ensure that health workers can reach their fullest potential as a way of ensuring effective and efficient performance from the workers.
According to a study by Willis-Shattuck and others (2008), findings showed that motivation concerning career development and training in the context of self-actualization according to Maslow’s hierarchy of needs is a very critical factor in as far as the performance of health-care workers is concerned. Health workers guided by intrinsic motivation factors have the desire to gain personal growth and more skills to enable them to perform better. If such training and educative opportunities that ensure professional growth are lacking, this is very demoralizing for the health workers and especially the young professionals. Professional development through training or education is very important because it allows health workers to handle job requirements in a more proficient manner.
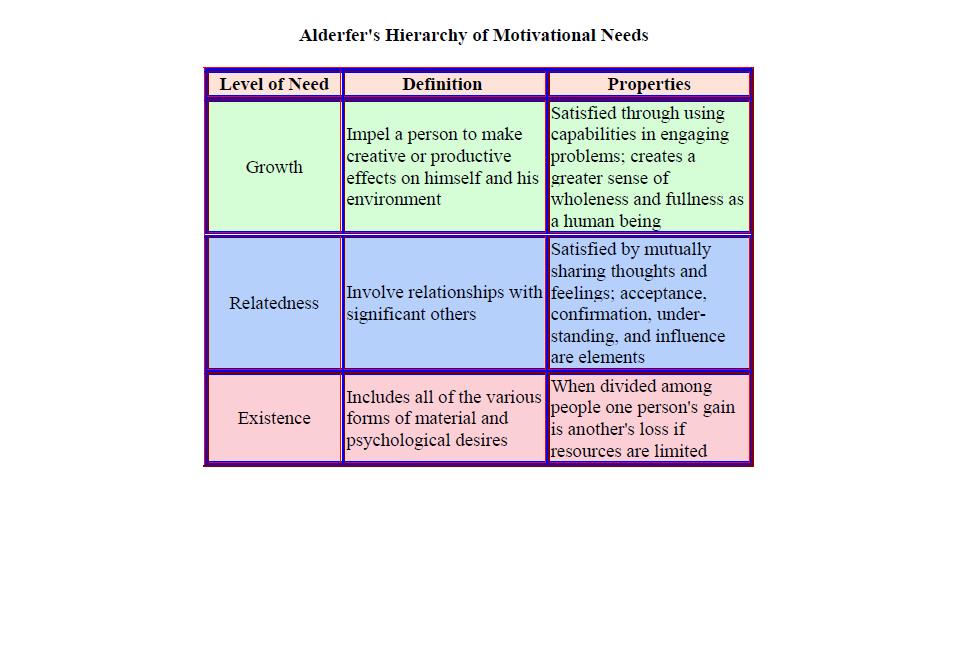
Alderfer’s Hierarchy of motivational needs is a revised version of Maslow’s hierarchy of needs where Clayton Alderfer linked Maslow’s hierarchy of needs with empirical research. After revising Maslow’s theory based on the hierarchy of needs, Alderfer came up with the ERG theory (Existence, Relatedness and Growth). Existence is in line with Maslow’s physiological and safety needs where an individual’s existence is concerned with the existence of basic materials. Relatedness is compared to Maslow’s social/love needs the external element of the esteem need. Relatedness is an individual’s desire to relate well with other people. Growth is synonymous with Maslow’s intrinsic component of the esteem need, as well as self- actualization (Murphy, 2009; WHO, 2006).
According to Alderfer’s hierarchy of needs, one focuses on increasing the satisfaction of a lower-order need when achievement of a higher-order need is frustrated. For example, when a health worker fails to satisfy his/her need for social interaction which is a higher-order need compared with catering for one’s material needs, the health worker results in regression to the lower-order material needs. Unlike Maslow’s theory, Alderfer’s theory shows that various needs can act as motivators simultaneously. The figure below gives a summary of Alderfer’s theory of needs (Dieleman & Harnmeijer, 2006):
Motivational Theories: Herzberg’s Two-Factor Theory
Another theory is Herzberg’s two-factor theory, otherwise known as motivation-hygiene theory. This theory was developed from a study that aimed to test the notion that people have two sets of needs:
- The need to eliminate pain as animals
- The need to grow psychologically as human beings
According to Herzberg’s study, there are two kinds of themes where each theme depicts a certain meaning concerning things that make people happy and those that do not make them happy. The first theme comprises of things that create motivation or job satisfaction and these are achievement, the work itself, responsibility, advancement and recognition. Work itself, advancement and responsibility are deemed to be of most concern concerning bringing about permanent changes concerning attitude. On the other hand, the second theme comprises on determinants of job dissatisfaction, which are working conditions, salary, company policy, supervision, administrative policies and interpersonal relations (Dolea & Adams, 2005).
Factors related to job satisfaction are separate and distinct from those that bring about job dissatisfaction. When health service managers remove dissatisfaction factors, this enhances peace but does not bring about motivation because the managers will be placating the workers instead of motivating them. It is because of this reason that Herzberg refers to the dissatisfaction factors as hygiene factors because when they are adequately present, health workers are neither satisfied nor dissatisfied thereby creating a hygienic and peaceful working atmosphere. Herzberg emphasizes that factors related to the work itself like “promotional opportunities, opportunities for personal growth, recognition, responsibility and achievement” as they are deemed to be intrinsically rewarding to the health workers (Dieleman & Harnmeijer, 2006).
In India, health workers regard motivating factors such as availability and accessibility to working tools, opportunities to train, suitable physical conditions and good working relationships with colleagues to be much more important than financial incentives thereby confirming Herzberg’s theory if the intrinsically rewarding factors (Peters, et al., 2010). This is in contrast to other regions like Ghana and as seen earlier in Malawi where financial incentives are the main reason why health workers are de-motivated thus according to Maslow’s hierarchy theory of needs, they have not yet satisfied their physiological needs (Agyepong, et al., 2004). There have been other findings to support this thereby; it is difficult to rule out non-financial motivating factors since better financial incentives alone cannot significantly enhance health worker motivation.
The working conditions are another factor that determines health worker motivation. The working conditions determine a health worker’s contentment concerning the working environment. The issue of working conditions does not merely include having adequate equipment and supplies; rather it also encompasses systems issues like information-exchange processes, decision-making processes and capacity issues like infrastructure, workload and support services (Potter & Brough, 2004).
Working conditions also entail protection against infectious diseases such as HIV and AIDs. Logically, poor protective mechanisms and facilities lead to escalated fears of infection and as a result, there is limited towards the provision of quality services and tasks are delegated to non-qualified staff (KIT/CHAZ, 2005; Dovlo, 2005). This eventually affects health service delivery and is associated with reduced health outcomes.
Availability and accessibility to hospital infrastructure and resources is a very important motivating factor for health workers. When health workers are not provided with adequate and essential equipment to work with like microscopes, then it becomes difficult for them to appropriately and adequately utilize their resources and as such, this acts as a great de-motivating factor. When a hospital lacks the necessary equipment, the health workers, alongside the patients, lack confidence and as a result, the health workers lose confidence in themselves and the patients, on the other hand, lose confidence in the health workers and the hospital at large. This can all be avoided if the health service managers understand that the intrinsic component of job fulfilment and satisfaction is very important concerning the provision of the required equipment and drugs by the health workers (Manongi, Marchant & Bygbjerg, 2006; Sararaks & Jamaluddin, 1999).
It always feels good when one’s efforts are recognized by their managers and/or supervisors, and he/she is motivated to work even harder. This case also applies to the health workers, who get motivated when they are recognized and appreciated by other people including the mangers, their employers and the outside community. This recognition and appreciation give the health workers the motivation and determination required to enhance their performance and deliver efficient and effective health services (Dieleman et al., 2006; Franco et al., 2004).
Motivational Theories: Expectancy Theory
The expectancy theory has been the most popular motivational theory in contemporary times. This theory has its origins in Victor Vroom’s work on motivation in 964 when he comes up with Vroom’s theory that is based on the presumption that behaviour is a product of conscious choices among alternatives aiming towards minimizing pain and maximizing on pleasure (Vroom, 1970).
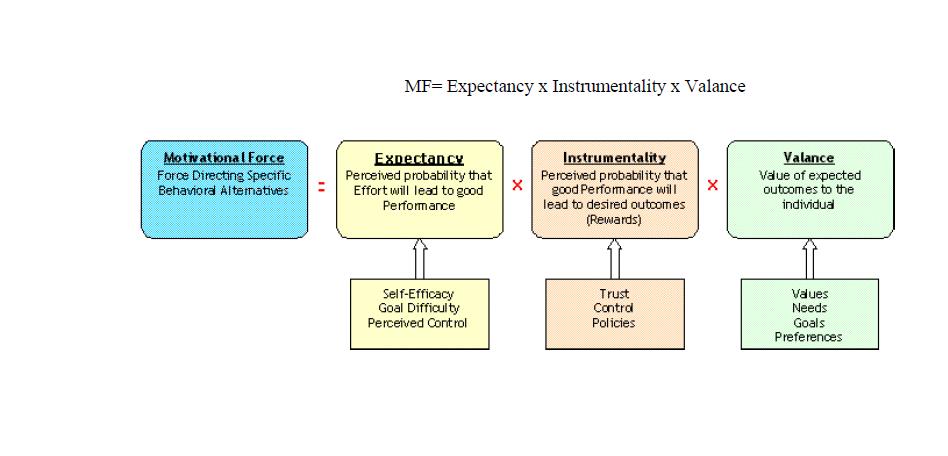
Expectancy, instrumentality and valence are the main components of this theory, where each component is associated with a particular belief. Expectancy is associated with the belief that particular job performance can be attained. In this case, health workers will be motivated to work if they believe that they are confident enough about the task at hand. The various factors influencing a worker’s expectation are: level of confidence in skills possessed concerning the task, support from superiors and subordinates, availability of critical information and quality of materials and equipment in place (Baumeister & Vohs, 2004; Fishbein & Ajzen, 1975).
Instrumentality is all to do with the outcomes of a task. In this case, an employee believes that high performance is important if certain outcomes are to be gotten. As a result, the health workers are motivated to work because they believe that performance is instrumental in as far as achieving a certain desired outcome is concerned (Lindner, 1998). Valence is based on the satisfaction that is expected from an outcome (Paul, 2009.). A worker is not motivated to work if the task is believed to yield into negative valence as opposed to a positive one. When none of the three conditions under expectancy theory prevails, then there is no motivational force for work. In summary, motivational force is equivalent to expectancy, instrumentality and valence as shown below (Cervone et al., 2006):
Other Motivational Theories
Yet still is another theory by David McClelland which states that workers are driven to work irrespective of their gender and culture by achievement, influence and affiliation. These drives are considered to be very crucial if the motivation is to prevail. Health workers are motivated to work effectively and efficiently if they can get results for their work, for example, achieving set goals and finding solutions to the problem.
Achievement of the desired result gives health workers the motivation they need to deliver effective and efficient healthcare services. In addition to achieving desired results and outcome, health workers are motivated by the need to belong to and interact properly with other health workers, their superiors as well as their subordinates. Influencing potential is another motivating element based on McClelland theory that is based on the need for power. Health service managers need to know which need is dominant for different individuals because the domineering need influences how an individual is to be motivated (Jones, 2008; MHEN & VSO, 2011).
The theory of X and Y by Douglas McGregor talks about two diametrically opposing viewpoints of managers concerning their workers. The theory of X is based on negative presumptions of the employees by the managers, for instance, an assumption that employees do not like to work and therefore must be forced, threatened and controlled so that they can do the work. On the other hand, the theory of Y is based on positive presumptions about employees like employees love to work and require no supervision for them to perform and work (Carver & Scheier, 2001). A health service manager should use the X and Y theories to positively influence the health workers and enhance their performance.
The goal-setting theory by Edwin Locke dictates that health workers are motivated by setting specific goals to direct their work. Goal commitment and self-efficiency are deemed to be the main influential factors in as far as the goal-setting theory is concerned (Gollwitzer, 1999). Other theories are reinforcement and equity theories. The reinforcement theory places attention on the factors that influence behaviour and these are the needs that have been discussed in the content of this paper in details (Cofer & Appley, 1967). Health workers will be motivated to work because of the need to achieve external factors such as reward other than internal elements as is the case with the goal-setting theory.
The equity theory revolves around balance/equity concerning motivation. In this regard, the equity theory is based on the perception of fairness as exercised by the management within an organization. The greater the fairness/equity perceived within an organization, the higher the motivation of the workers and vice-versa (Lu et al., 2005). Health service managers need to understand that they should give equal kind of treatment to all health workers of an equivalent cadre without favour. Health workers need to know that their inputs are equally appreciated and none is subjectively considered to be better than that of another worker.
Conclusion
The fact that health workers are an integral part of any health institution is irrefutable. Unfortunately, most health service managers fail to develop appropriate strategies to motivate different health workers. It is worth noting that health workers have different needs that trigger their motivation to work thus it is necessary as a health service manager to ensure that most of them are met to avoid issues of emigration that further aggravate the situation (Benson & Dundis, 2003). Developing countries are mainly faced with this huge challenge of retaining their health workers since most of these workers immigrate to developed countries where they are assured of better incentives alongside other improved non-financial incentives (MHEN & VSO, 2011).
Although developing/low and middle-income countries have constrained resources, strategies that facilitate personal growth and motivation within a local context is imperative. Health service managers need to understand that the needs of the health workers vary because different health workers may be interested in different kinds of needs based on their ability to satisfy them. When a health service manager understands what the health workers require based on their needs, then he/she can put in place the appropriate strategies that will act as motivating factors for the workers while applying the motivation theories discussed above (Dieleman, M., & Harnmeijer, J. W., 2006).
References
Agyepong, I., et al., 2004. Health worker (internal customer) satisfaction and motivation in the public sector in Ghana. International Journal of Health Planning and Management, 19, 319-336.
Baumeister, R. F. & Vohs, K.D, 2004. Handbook of self-regulation: Research, theory, and applications. New York: Guilford Press.
Benson, S. G., & Dundis, S. P., 2003. Understanding and Motivating Health Care Employees: Integrating Maslow’s Hierarchy of Needs, Training and Technology. Journal of Nursing Management, 11, 315-320.
Carver, C. S., & Scheier, M. F., 2001. On the self-regulation of behavior. New York: Cambridge University Press.
Cervone, D., et al., 2006. Self-Regulation: Reminders and Suggestions from Personality Science. Applied Psychology: An International Review 55 (3), 333–385.
Cofer, C. N, & Appley, M. H. 1967. Motivation: Theory and Research. London: John Wiley & Sons.
Deci, E. L., & Ryan, R. M., 2000. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemporary Educational Psychology, 25, 54-67.
Dieleman, M., et al., 2006. The match between motivation and performance management of health sector workers in Mali. Human Resources for Health, 4, 2.
Dieleman, M., & Harnmeijer, J. W., 2006. Improving Health Worker Performance: In search of Promising Practices. Geneva: Department of Human Resources for Health. Web.
Dolea, C., & Adams, O., 2005. Motivation of health care workers: review of theories and empirical evidence. Cahiers de Sociologie et Démographie Médicale, 45 (1), 135–161.
Dovlo, D. 2005. Wastage in the health workforce: some perspectives from African countries. Human Resources for Health, 3, 6.
Franco, L. M., Bennett, S., & Kanfer R. 2002. Health Sector Reform and Public Sector Health Worker Motivation: A Conceptual Framework. Social Science & Medicine, 54 (8), 1255-66.
Fishbein, M., & Ajzen, I., 1975. Belief, attitude, intention, and behavior: An introduction to theory and research. Reading, MA: Addison-Wesley
Garcia-Prado, A. 2005. Sweetening the Carrot: Motivating Public Physicians for Better Performance. The World Bank, Policy Research Working Paper 3772.
Gray, B., 1991. Are California Nurses Happy? California Nursing, 13, 12-17.
Gollwitzer, P. M., 1999. Implementation intentions: Strong effects of simple plans. American Psychologist 54, 493–503.
Hughes, R. L., Ginnett, R.C., & Curphy, G. J., 2002. Leadership, enhancing the lessons of experience. New York: McGraw-Hill/Irwin.
Jones, I. 2008. The Human Factor: Inside the CIA’s Dysfunctional Intelligence Culture. New York: Encounter Books.
King, L. A., & McInerney, P. A., 2006. Hospital Workplace Experiences of Registered Nurses that have Contributed to their Resignation in the Durban Metropolitan Area. Curationis, 29 (4), 70-81.
KIT/CHAZ, 2005. Coping with the impact of HIV/AIDS on health workers in Zambia: a pilot study in two districts. Amsterdam: Royal Tropical Institute.
Lu, H., While, A. E., & Barriball, K. L., 2005. Job satisfaction among nurses: a literature review. International Journal of Nursing Studies, 42, 211–227.
Manongi, R., Marchant, T., & Bygbjerg, I. C., 2006. Improving motivation among primary health care workers in Tanzania: a health worker perspective. Human Resources for Health 2006, 4 (1), 6.
Marsden, D., French, S., & Kubo, K., 2000. Why does Performance Pay De-motivate? Financial Incentives versus Performance Appraisal. London: Centre for Economic Performance. Discussion Paper 476.
Maslow, A. H., 1954. Motivation and Personality. New York: Harper and Row.
MHEN & VSO, 2011. Valuing Health Workers: Implementing Sustainable Interventions to Improve Health Worker Motivation. Web.
Murphy, J. 2009. Inner Excellence. New York: McGraw-Hill.
Paul, F. 2009. Health Worker Motivation and the Role of Performance Based Finance Systems in Africa: A Qualitative Study on Health Worker Motivation and the Rwandan Performance Based Finance Initiative in District Hospitals. London: DESTIN.
Peters, et al., 2010. Job Satisfaction and Motivation of Health Workers in Public and Private Sectors: Cross-sectional Analysis from two Indian States. Human Resources for Health, 8, 27-37.
Potter, C., & Brough, R., 2004. Systemic capacity building: a hierarchy of needs. Health Policy and Planning, 19 (5), 336–345.
Rowe, et al., 2005. How can we achieve and maintain High-quality Performance of Health Workers in Low-Resource Settings? The Lancet, 366, 1026-35.
Sararaks, S., & Jamaluddin, R., 1999. De-motivating Factors among Government Doctors in Negeri Sembilan. Medical Journal of Malaysia, 54 (3), 310-319.
Vroom, V. H., 1970. The Nature of the Relationship between Motivation and Performance. In Vroom, V. H., & Deci, E. L., Eds. Management and Motivation. Tennessee: Kingsport Press Inc.
WHO, 2006. Working together for health. Geneva: World Health Organization.
Willis-Shattuck, M., et al., 2008. Motivation and Retention of Health Workers in Developing Countries: A Systematic Review. BMC Health Services Research, 8, 247.
Zurn, P., Dolea, C., & Stilwell, B., 2005. Nurse retention and recruitment: developing a motivated workforce. Geneva, World Health Organization.