Introduction
Animal bodies contain chromosomes that carry DNA segments called genes. Genes are important, in that, in human beings, genes determine characterization. For example, genes determine the hair color, loftiness, and heaviness of human beings. Moreover, genes are paramount in establishing behavior patterns and personalities in human beings. Nevertheless, genes have one most imperative aspect; the capacity to pass on genetic disorders and diseases from one human being (parent) to another (offspring). Such diseases and disorders emanating from idiosyncrasies or incongruity in genes or chromosomes identify as genetic disorders. Biologically, genes are small building blocks that structure DNA, the fundamental entity of life. Thus, idiosyncrasies in genes, result in alteration of gene appearance. Consequently, diverse genetic modifications, for example, the union of two recessive genes, might lead to genetic diseases or disorders. On the other hand, direct contact with radioactive emissions and rays can lead to genetic disorders. Today, scientists have managed to discover more than 4000 genetic disorders affecting human beings worldwide. These genetic disorders fall into four major classes. The first class, single-gene disorder, occurs when there is a mutation within a single gene. Genetic disorders like hemophilia, cystic fibrosis, and sickle cell anemia fall into this category and can pass from parent top progeny. Other categories include chromosomal abnormalities, multifactorial and mitochondrial (mitochondrial DNA) mutations. The paper will examine hemophilia as a genetic disease.
Hemophilia: Description
Hemophilia is a genetic disorder of the blood. Normally, hemophilic patients’ blood fails to clot. If an injury occurs on the body leading to the cutting of the skin, hemophilic patients can bleed longer than non-hemophilic persons can. Scientific research shows that this genetic disorder can also lead to internal bleeding especially in the joints hence, destroying other body tissues or organs. Since hemophilia is a genetic disorder, it passes down the family lineage via genes. Persons having hemophilia lack the clotting factor (protein need), which will collaborate with platelets for blood to clot. The role of the clotting factor is to gum platelets together and bung the injury area. Thus, minus clotting factors, there is nothing to block the injured area to control blood from oozing out. Nevertheless, through injections with clotting factors, hemophilic persons can stop bleeding. Due to its dissimilar nature, scientists classify hemophilia into two types. The first type is hemophilia A where persons have nil or squat amount of clotting factors (F8). Interestingly, the majority of hemophilic persons, in fact, 90 percent, have hemophilia A. on the other hand, the second type of hemophilia is, hemophilia B, which is characterized by the absence or diminutively low levels of clotting factors (F9). (Dimitrios, Zaiden & Saduman, 2004, Para. 1-7)
Causes of Hemophilia
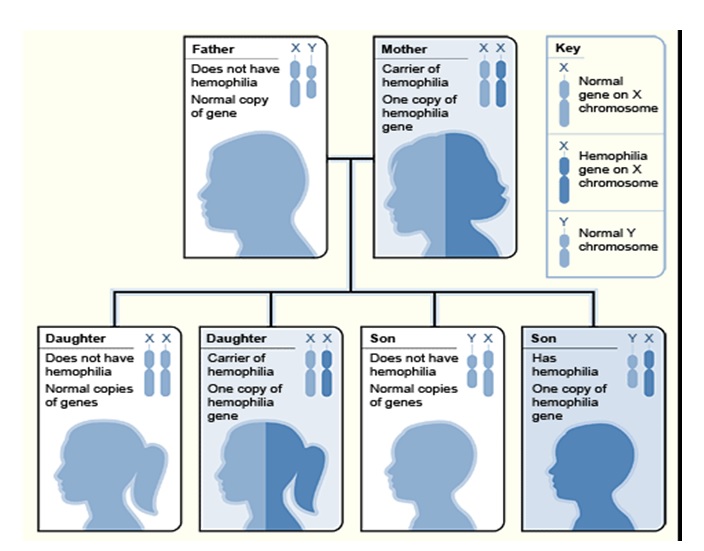
Without any further deliberation, a human being having hemophilia through inheritance was born with this genetic disorder. So many people do not understand the real cause of hemophilia. Nevertheless, hemophilia like any genetic disorder occurs when there is imperfection within genes vital in the production of blood clotting factors F8 and F9. The X chromosomes are the ones, which accommodate these particular genes. Coincidentally, there is no single chromosome but instead, chromosomes appear in twosome. Genetic research indicates that female human beings have one pair of X chromosomes. On the other hand, male counterparts boast a single X and a single Y chromosome. However, only genes contained in the X chromosome, recount to clotting factors. Male human beings are vulnerable to this genetic disorder in that, any gene idiosyncrasy in the X chromosome results in hemophilia. In contrast, the scenario is different in female human beings in that, it requires gene abnormality in the two X chromosomes to be hemophilic; cases that scientists term infrequent. Nevertheless, in a scenario where there is an anomalous gene in a female human being, then she behaves as a “carrier”. (U. S Department of Health and Human Services, 2009, Para. 1-5).
Nonetheless, this particular person is not in any danger as the remaining X chromosome contains clotting factors instrumental in blood clotting. The only disadvantage with her is that the genes can pass to her children. Under very rare occasions will a baby girl be born hemophilia. If it does happen, then the mother has carrier genes and the father is an automatic hemophilic. Sometimes, some females bear hemophilic male children even when they are not carriers. Genetic research shows that the genes might have undergone random change or mutation before transferring into this male child. The random change in the clotting factors F8 and F9 cause hemophilia A and hemophilia B respectively. (U. S Department of Health and Human Services, 2009, Para. 6-8).
Signs and Symptoms
The two main hemophilia signs and symptoms include effortless bruising and largely, excessive bleeding. Nevertheless, some hemophilic persons bleed excessively than others. This is because; there are persons who have mild hemophilia (less bleeding), and others have severe hemophilia, which results in excessive bleeding internally or externally when there the skin injures. Other signs of hemophilia include internal bleeding in the mouth, knees, elbows, and other jointed sites. Peculiar signs of hemophilia include blood in urine and stool because of bleeding in the kidney and intestines respectively. Unexpected nosebleeds and blood in the mouth even with a minor cut are clear signs of hemophilia. Continual vomiting, clumsiness, headaches, double vision, and convulsions can also be signs of hemophilia causing bleeding in the brain. (National Hemophilia Foundation, 2006, Para. 1-8).
History of Hemophilia
It was during the Babylonian Talmud when a biological reader and researcher, Rabbi Judah haNasi shed light on the existence of hemophilia. He worked on the idea that, if one circumcises his children one by one and they all die due to excessive bleeding, then there is a likelihood of hemophilia targeting along the family lineage. However, in the tenth century, Albucasis, a medical practitioner, associated families that loose male members because of excessive bleeding with hemophilia. Scientific analysis on hemophilia started in the 19th century. A scientist from Philadelphia, Dr. Jon Conrad showed how hemophilia passes from parents to progeny by studying his folks. From his discovery, males were in great danger of inheriting hemophilia than females. In the mid-twentieth century, Harvard doctors, Taylor and Patek, came up with an anti-hemophilic globulin that acted as clotting factors. Ten years later, a medical practitioner from Buenos Aires, Pavlosky, performed a series of lab tests on blood samples and found out the two types of hemophilia; hemophilia A and hemophilia B. Additionally, he found out that, if two hemophilic persons exchange blood, the genetic disorder reverses, hence; different types of hemophilia. (Handin, Lux & Stossel, 2003, pp. 1167-1182).
Diagnosis of Hemophilia
Persons suspecting to have hemophilia along with their families should opt to go for medical examination. Doctors take blood samples to identify the level of clotting factors and the time or period, which blood takes to clot. Consequently, persons will understand whether they are hemophilic, and if so, its type and severity. After the test, persons with hemophilia A or B have mild, moderate, or severe hemophilia symptoms. This is because, the level of clotting factors, F8 and F9 vary from one person to another. Scientific research shows that, persons with mild and moderate hemophilia A or B exhibit similarities in bleeding. Luckily, babies born with hemophilia can diagnose one year after birth, unlike mild and moderate hemophilic persons who wait up to adulthood for doctors to carry out an effective diagnosis. Medical advancements have seen doctors carry out hemophilia tests on suspected hemophilia carriers, who happen to be expectant women, within the first ten weeks of pregnancy. In case of any danger, medics carry out a preimplantation diagnosis to free the child from hemophilia. (Ferrata Sorti Foundation, 2004, pp. 1036-1037).
Treatment of Hemophilia
Although a genetic disorder, medics can treat hemophilia by replacement therapy. Here, medical practitioners inject anti-hemophilic globulins rich in clotting factors F8 and F9 for hemophilia A and hemophilia B respectively. The concentrates manufactured from human blood, add to the missing or low levels of clotting factors within the X chromosome. Other treatments include an inoculation or nasal neuter of Desmopressin (DDAVP), a hormone that can reverse symptoms produced by mild and moderate hemophilia A. Unfortunately; this particular hormone is not effective in severe hemophilia A and hemophilia B persons. There are also other antifibrinolytic medicines, which treat hemophilia. For example, tranexamic acid or aminocaproic acid together with replacement therapy, can add clotting factors to X chromosomes and stop internal bleeding. (Roosendaal & Lafeber, 2007, pp. 603-605).
Prevalence in the U.S. and the World
Hemophilia persons can be found everywhere in the world. In the United States alone, there are over 18,000 people with hemophilia, and each year, doctors report 400 cases of born babies with this genetic disorder. It is quite clear that, since males have only one X chromosome, they are vulnerable to hemophilia than females who need abnormality in both X chromosomes for them to test hemophilia positive.
Reference List
Dimitrios, P., Zaiden, A., & Saduman, O. (2004). Hemophilia Overview. Web.
Ferrata Sorti Foundation. (2004). Molecular basis of von Willebrand disease and its clinical implications. Haematologica, 89 (9), 1036-1037.
Handin, I., Lux, E. Stossel, P. (2003). Blood: principles and practice of hematology. Philadelphia: Lippincott Williams and Wilkins.
National Hemophilia Foundation. (2006). What is a bleeding disorder? Web.
Roosendaal, G. & Lafeber, F. (2007). Prophylactic treatment for prevention of joint disease in hemophilia-cost versus benefit. New England Journal of Medicine, 357 (6), 603–605.
U. S Department of Health and Human Services. (2009). What Causes Hemophilia? National Heart, Lung, and Blood Institute. Web.