Introduction
Technology has become one of the most important aspects of healthcare in the modern world bearing in mind that it has been embraced extensively. In this regard, it has been integrated into various operational functions in the Indian healthcare information system. New programs have been developed continuously to solve the upcoming challenges in the healthcare arena (Eswarappa 178). Having solved some of these challenges, the technological programs have simplified the processes of treating diseases as well as the interaction between doctors and patients (Eswarappa 347). Based on this understanding, this paper will thus focus on the various technological developments that have been incorporated into the healthcare system with the help of computers and other devices.
Besides technology, it is essentially crucial to focus on the healthcare setup and how it is aligned to the level of illness in India. This undertaking can be accomplished by determining whether the healthcare providers consider illness when they are setting the various aspects of the healthcare system. In an attempt to make this crucial determination, this paper will also discuss some critical illnesses, such as HIV/AIDS, environmental causes, and disability, and compare them with the healthcare provisions. As a result, there are two distinctive objectives of this paper according to the above elucidations.
- To discuss the technological advancements in the Indian healthcare system.
- To determine whether Indian healthcare considers illness during the process of planning.
Technological Advancement of Indian Healthcare
The technological aspects of Indian healthcare has undergone a profound transformation, especially when it comes to information systems. In the recent past, the Indian healthcare system relied on the manual execution of roles and the physical presence of the professional. However, technology has brought new experience and development to the Indian healthcare system whereby patients can be monitored without the bodily presence of the practitioners and clinicians. The subsequent paragraphs discuss some of the improved systems that are used to accomplish the manual roles in the quest to reach more people in society.
Telemedicine Technologies
One of the most crucial technological innovations that have been conceived in the healthcare information system of India is the telemedicine program. It is evident that most of the physicians in India reside in urban areas while the others live in rural areas. Particularly, it is established that 3 percent of the clinicians live in the villages while 25 percent reside in the semi-urban areas and the rest in the towns (Khoumbati 174). This implies that the number of physicians who are available for the people in rural areas is essentially negligible. Telemedicine is a program that uses mobile phones to track the progress of patients in different parts of India such that the doctors do not need to leave the hospital premises. In addition, it reduced the need for patients to leave their residences and visit the hospitals for diagnoses. Through this program, the doctors can give a drug prescription, advise the patient about some health issues, or diagnose while the patient is still at home.
Among the fundamentally vital developments that have taken place in the program is the introduction of the mobile monitoring system. This program has been conceived by a student in one of the Indian universities known as Loughborough and some professionals in the telemedicine arena (Khoumbati 129). The program is a very innovative system that enables health professionals to track the health of patients using mobile phones. The mobile phone is capable of taking and transmitting information concerning various health aspects, including blood pressure and blood sugar. Having collaborated with other universities, the phone has been developed to make the special mobile phone more portable and powerful in terms of transmitting the information.
Apollo Hospital’s ICT Initiative
Apollo Hospitals are committed to transforming Indian healthcare in collaboration with Cisco. In their attempt to fulfill their objective, the first step involves leveraging the ICT system in order to integrate it with the operations of Apollo Hospitals. In addition, the first phase involved the development of the Cisco Health-Presence initiative. The second step in their program involves undertakings that seek to develop and improve the technological standards in that attempt to transform the entire healthcare. In their third step, the Apollo initiative seeks to leverage ICT in order to provide solutions to the problems facing health care not only in India but also in other parts of the world that include Asia-Pacific and developing countries (Khoumbati 176). The Extended Reach program will enable the health practitioners to provide services in the entire country with ease in contrary to the past years where the physicians have been forced to attend to the patients physically.
Center for Development and Advanced Computing Technologies
In the past, the rural areas had been abandoned as far as healthcare attention was concerned. Besides the aspect of few physicians in rural areas, it is evident that India has a huge population that makes it difficult for the physicians to attend to all the people satisfactorily. For this reason, CDAC has developed Infothela software to facilitate the exchange of patients’ information. The system comprises both the back-end and front-end sides that help in executing different roles. The latter depends on the non-medicine experts who collect information from the patients and then transfer it to the former. The back-end is monitored by medicinal specialists who interpret the sent information, make conclusions, and diagnose by prescribing the necessary treatment. Infothela program, which is powered by a computer system, involves the use of the Internet, emails, and mobile devices when collecting information as well as administering treatments.
In regard to the development of infothela, the center for Development and Advanced Computing began working on the project in Bangalore where they sought to use it for primary care (Khoumbati 156). While accomplishing the undertaking, the specialists incorporated the database system and the information about the interaction between patients and doctors. Further, the two components were combined with the web-designed system of management, text-messaging and other web programs among others. Having considered the extensive use of mobile phones in India, the developers have been working to make a wireless application that can enable the integration of this system with these devices.
Further, CDAC has developed a program known as ONCONET that is involved in capturing, storing, transmitting and processing images using web-based systems. This software comes as a development of the telemedicine arena since it can be used to capture and transmit pictorial information from the patients to the doctors without physical appointments. It has been implemented to enable the operation of the ACI telemedicine networking system. In essence, CDAC has developed a total of eight technological programs that are set to improve the field of telemedicine (Khoumbati 127). The eight programs are focused on specific fields of medicine and aim at solving the problems that are related to those areas.
Health Management Information System
This is a system that was developed by ICTPH and another technology company known as Swath India. This system incorporates all the aspects of managing the healthcare sectors by using features that are easily integrated with other technologies. The system obtains data from three different external sources that include diagnoses, mobile technology and survey studies. In regard to diagnoses, HMIS obtains data from the previous treatment that have been prescribed by the doctors. The diagnostic data includes aspects such as blood pressure, CBC, and body chemical analysis. When it comes to mobile technology, it has been integrated into the system to focus on young children within the range of 2 to 24 months of age. For example, information concerning nutritional cases is collected using portable devices and recorded in the HMIS.
Importantly, it seeks to eliminate the health menaces conjoined to anemia that is caused by a deficiency of iron in the body. When collecting this information, the caregivers use mobile phones to conduct surveys and get helpful data concerning health issues. In addition, HMIS depends on the surveys that are conducted with the help of well-designed questionnaires. These questionnaires are scanned using unique technological devices that are incorporated in the HMIS to collect information about the patients. Particularly, the questionnaires are scanned using the Optical Mark Recognition and fed into the back-end to gather statistics. However, the rising use of mobile devices has been replacing the use of scanned questionnaires gradually.
HMIS Features
The HMIS comprises a demographic section that captures data related to the various individual aspects, including age, gender and geographic location among others. Most of the information stored in this part of the system grows organically so that the patients’ data is captured accumulatively as they continue visiting the hospital. Once the information is obtained, the HMIS organizes it into groups according to geographical entities and households (Swaminathan 143). In addition to the demographic section, HMIS comprises the outpatient module that is the most-used part of the entire system. This part accomplishes various tasks, including the provision of interfaces for clinical practitioners, moderation of individual information, and assignment of the location to the mentioned healthcare providers.
Health Care Consideration of Illness
Status of HIV Illness and Its Consideration in Healthcare
Unfortunately, the projections that can be made in regard to the future status of Indian health are notoriously uncertain. Nonetheless, the future status of Indian health rests on the general transformation of its political prospects that have been implemented in the quest to reduce poverty and mitigate its effects. In essence, the ability of people’s capability to pay for healthcare services will affect their willingness to take responsibility for their own health. In addition, the government’s commitment to the effective dissemination of public information will also determine the ability of the citizens to take preventive measures. Importantly, the future level of morbidity will also be determined by the consciousness of the government and the private sector on the vulnerable people in the society, nutritional awareness, and women’s empowerment. It thus follows that if these are the pertinent aspects that will impact the level of morbidity, the question of whether the Indian healthcare system considers illness during planning must revolve around them. In particular, there are various forecasts that have been made in relation to the future status of the illness. One of these forecasts relates to the deadly HIV/AIDS that has posed a great challenge and menace to the entire world. In one of the research conducted by the World Health Organization, the results showed that there can be a critical decrement in the level of HIV/AIDS prevalence if the healthcare system will be diligent on vaccination.
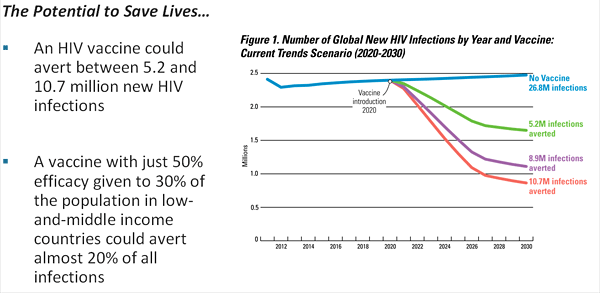
In this projection, it is evident that the HIV/AIDS vaccine can avert about 5.2 and 10.7 million additional infections that can arise from 2020 to 2030. If there is no vaccine applied completely, the country can suffer 26.8 million new infections (Ambedkar 124). This implies that when the vaccine is not applied, the rate of infection is even much higher than the way it can prevail without vaccine intervention.
In addition, the minister convened a meeting with all the stakeholders to determine the positive and negative impacts of implementing the policy in the healthcare system. A legislator known as Shirish Shinde had presented a motion in the parliament arguing that the projection showed a high probability of increasing numbers of people living with HIV (Ambedkar 157). He argued that the probable increase of PLWHA required the state to act boldly and swiftly in order to control the menace. In this regard, it is evident that the legislator was considering the possible level of illness during his proposition. A similar sentiment was elucidated by the minister women and children’s development where she argued that the level of HIV/AIDS prevalence in India reached alarming rates. Furthermore, she stated that the future projections were not favorable since there was a possibility of increased rates of the disease prevalence. This implies that the minister’s decision to propose the bill with the help of a legislator was based on the fact that the rate of illness was predicted to rise in the future. The minister thus believed that the state needed to curb the rising rates of the disease among the people. In addition, this was inspired by the fact that people had shown reluctance in regard to taking the tests voluntarily. This shows that the administrators and other pertinent stakeholders were concerned about the illness, in regard to HIV/AIDS, when making their policies. In essence, this can be considered as the culture of the mentioned stakeholders when it comes to matters of developing and planning the healthcare system in India.
Healthcare Consideration of HIV/AIDS
Further, in order to determine the extent to which the involved stakeholders consider illness when planning for their healthcare system, it is essentially important to focus on the awareness of HIV/AIDS in India and compare with the above statistics. The comparison will show whether the stakeholders are considering the level of illness when conducting their awareness campaigns. In essence, this is based on the premises that if they consider the high expected rates of HIV/AIDS infection, the campaigns should be intensified and satisfactory.
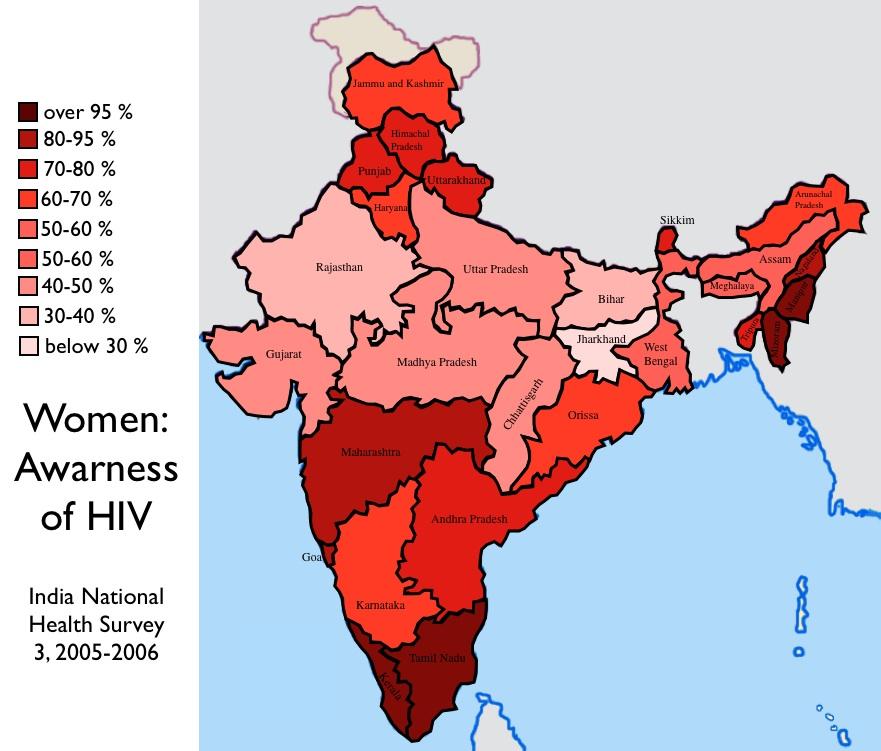
In the above results, it is evident that the largest part of India comprises of women whose awareness on HIV/AIDS is between 40-50 percents. This implies that the government has not attained satisfactory levels of awareness in regard to the prevalence of illness. Bearing in mind that the future projection that was presented in first diagram predicted a 5.2-10.7 million increase in the level of HIV/AIDS by 2030, the state should have considered this and intensify the level of awareness among women. In this regard, we consider women since they are most vulnerable to the level of HIV/AIDS. In respect to the campaign and awareness concerning the disease, the stakeholders have not considered the level of illness while implementing their awareness programs.
Personal Opinion about Women awareness on HIV/AIDS
The awareness of women about illness is an essential factor when it comes to improving the Indian healthcare. This importance is based on the premises that women are among the members of the population who are confronted by a higher risk of contracting diseases. In addition, women are considered as crucial people when it comes to taking care of the family and the children. This implies that women are not only critical to their health, but also crucial to the welfare of the family in respect to hygiene, eating habits and other aspects that concern health. When it comes to the above discussion concerning HIV/AIDS illness and mortality occasioned by this disease, women must be involved actively to ensure that the battle against the disease is won. This becomes critical when because the vaccination of young children against the epidemic relies on the diligence of their mothers. If the mothers are sensitive about the importance of vaccinating and protecting their children against the disease, it becomes easier to reach the children and to protect them. On the other hand, if they are not aware, it becomes difficult to reach the at-risk population that mainly includes young ones.
Status of Illness Regarding Disability and it consideration in Healthcare
Besides HIV epidemic, disability forms another critical aspect of the illness among the Indian people. Indeed, when discussing illness, it could be completely inappropriate to disregard disabilities (Eswarappa 118). In essence, disabilities affect a substantial part of the population. The disabilities take many forms, including the mental and physical disabilities. In order to maintain the objective of this discussion, it is important to recall that the main aim is to determine whether illness is considered when planning the healthcare. In an attempt to make this determination, this section will analyze the status of disabilities and then determine whether the healthcare has been positioned to address these disabilities in relation to their prevalence. As a result, the comparison can help to adjudge whether the healthcare is conscious of illness status or not.
These demographics present the status of disability in India according to various aspects such as age, sex, and the extent of severity among others. The purpose of presenting these demographics and analyzing them is to form the basis of comparing with the healthcare provider and determine whether the illnesses were considered when planning the healthcare system. According to the census and NSS, the population of people with disability comprised 2.1 and 1.8 percent respectively. Whereas this is a very small portion when it is viewed in terms of percentage, the real population accounts for about 18 to 21 million people (Sorajjakool, Carr & Nam 197). This implies that the healthcare system of India must venture to consider these people when planning their healthcare system. According to the male and female results, it was evident that the number of women affected by disabilities was less than men. It was estimated by NSS that, for every 1000 men, there are 698 disabled men. On the other hand, the census established that there are 738 women affected by disabilities for every 1000 men (Thapa, Aalsvoort & Pandey 373).
Healthcare Consideration of Disabilities
Having analyzed the prevalence of people with disabilities within the country, the analysis of healthcare facilities is crucial for making a comparison. In Taluk village, there is research that was conducted to determine the extent to which the people of that village accessed medical facilities. When identifying the problem that inspired the research, the author stated that most of the health facilities are located in urban areas while most patients who need the services reside in rural areas. After conducting the research, they established that most of the disabled people in the rural areas were capable of taking care of themselves without the use of supportive devices. Further, it was discovered that about 13 percent were severely disabled, and they could not use the appliances. They noted that about 50 percent of the disabled people who needed medical attention were able to reach the facilities. However, the research established that the rehabilitation services were not effective in the village. Another research that had been conducted in Bangladesh showed that 98 percent of the visually challenged people had not used spectacles. On the other hand, 96% of the people who had a hearing problem did not use the appliance to mitigate their physical challenge. These analyses show that there are insufficient disability-based health facilities in rural areas. Nonetheless, 75% of the people with disabilities live in rural areas such as Takul. This comparative analysis shows that the government has not aligned the healthcare facilities in accordance with the illnesses occasioned by disabilities.
However, there are health-related provisions that have been stipulated to coincide with the aspects of disabled people. In this case, the government has ensured that the children with mental and physical afflictions have access to special education institutions that have training facilities. The government has provided professional trainers who take the students through programs that help them to recover their mental capability.
Personal Opinion on the Status of People with Disabilities
The people with special needs have been regarded as a minor portion of the population. They are not considered to pose a major problem to the healthcare of India. However, this is a dangerous and insensitive approach towards managing healthcare. The healthcare act that was stipulated in 1995 gave disabled people the right to live normally. It has provided children with the right to attend school and to have access to medical facilities. It has stipulated that children with special needs should be granted a certificate to access these facilities. This act recognized the importance of upholding the rights of disabled people. As a result, it is out of order for the government to marginalize these people and consider them as minors. Indeed, despite their small population, their interests are essentially pertinent to the welfare of the country (Singh 134).
Importantly, the government and other concerned authorities should be concerned about the medical facilities in the rural areas. In this case, it was discovered that most of these people are in rural areas. As a result, the medical facilities should not be concentrated in urban areas. Instead, they should be decentralized and brought to the rural areas so that a substantial number can access them easily. This will improve the healthcare system profoundly based on the premise that the medical facilities will be serving the people satisfactorily.
Status Illnesses Caused by Environmental Aspects
Diseases that are caused by environmental aspects are very crucial when it comes to matters of illnesses. In this case, this discussion will consider the various diseases occasioned by environmental hazards and compare them with Indian healthcare to determine whether the system has considered them. The comparison will bring out the risk factors and environmental diseases and show how they are curbed or ignored in the country. The table below shows some of the risk factors and the expected impacts on the population’s health.
A research conducted by WHO in India revealed that the total burden of diseases caused by the environmental factors accounted for 24 percent of the illnesses. This was equivalent to a total of 2.6 million deaths per year. While considering the specific rates of morbidity in relation to India, the following statistics were released by the World Health Organization.
It is evident that India is confronted by critical illnesses, including neuropsychiatric disorders, cardiovascular disease, and musculoskeletal afflictions and asthma. Although there are other diseases affecting the country, these have a high rate as compared to the world’s highest and lowest recorded percentage of prevalence.
Healthcare Consideration of Environmental Illnesses
In essence, these are various illnesses that have been considered while setting up the healthcare of India whereas others have been ignored. India has produced highly qualified professionals to cope with the challenges posed by cardiovascular and musculoskeletal diseases. This is a step showing that the country has considered the level of illness when planning the healthcare facilities. However, they have disregarded asthmatic diseases because there are very few regulations that have been stipulated to control the causative agents of asthma, such as dust, the level of humidity and storms. For example, the country could have planted trees that break the strong storms in order to curb the level of dust in the air. In addition, the use of motor vehicles has contributed extensively to the prevalence of asthma due to the emission of Carbon IV Oxide (Sarkar & Panigrahi 129). The Carbon IV Oxide has a profound effect on asthmatic people who are vulnerable to the disease. In this regard, there should be policies that control the emissions of this gas and other particles that make cause asthma. In regard to diarrhea, there are pools of dirty water all over the country especially in places such as Tamil. The pools are occasioned by the high levels of convectional rainfall received in this region. The water pools cause the diarrheic condition to prevail in this region while the healthcare system does not consider this condition during the planning. In fact, the water does not only cause diarrhea, but also malaria prevalence within the region. This is because malaria is caused by mosquitoes that breed in dirty dirty water and infect people. Besides the water is dirty, there are landfills that accompany it making the situation worse.
Personal Opinion on the Environmental Diseases
In essence, the diseases caused by environmental conditions are very harmful to the welfare of Indian conditions. In this regard, there have been profound deaths that are caused by poor sanitation in households and public places. As a result, the people of India must take the initiative to curb this menace. First, the citizens should ensure that they maintain good hygiene in order to curb diarrhea and other related conditions. In addition, they should ensure that all the landfills are eliminated to remove the breeding areas for mosquitoes. Landfills do not only form the breeding places for the mosquitoes but also pose other dangers to the health of the people living around them. These dangers include aspects such as physical injuries bearing in mind that some of the landfills contain metallic objects. These objects are responsible for the injuries that can pave way for other diseases and illnesses caused by pathogens. In that regard, it becomes a chainlike process that leads to poor health conditions among the citizens. In general, the Indian healthcare stakeholders should pay attention to the vaccination against HIV/AIDS and the creation of awareness among the people. This will help to reduce the impact of the disease since it is projected that the vaccination can avert about 20 percent of the possible additional victims. In addition, people with disabilities should not be considered as minors since considering their afflictions is pertinent to the attainment of a proficient healthcare system. The environmental conditions should be considered in equal measures when designing the healthcare arena. This is based on the fact that there are considerable cases of mortality caused by the environment-based diseases.
Conclusion
India has been capable of integrating technology in their healthcare system profoundly and effectively. CDAC has been at the forefront of developing software and programs that enable the doctors to reach many people in the country. In this regard, special mobile phones that have the software can transfer information to the healthcare practitioners in order to get advice or treatment. As a result, doctors do not necessarily attend to the patients physically since they can accomplish the task through technology.
It is evident that the healthcare system of India is substantially consistent to the level and type of illnesses prevailing in the country. This consistency is caused by the commitment of all stakeholders towards eliminating various illnesses around the country. For example, they have shown a willingness to create awareness among women concerning the HIV/AIDS. This is an important step because women comprise of an important part of the population that does not only determine its own welfare, but also the health of the family members.
On the other hand, they have neglected various areas such as the construction of healthcare facilities in rural areas for people with disabilities. In addition, the government has not paid much attention to the elimination of landfills that pose a major threat to the health of the citizens. In this regard, landfills create breeding grounds for the mosquitoes and hence support the prevalence of Malaria. Further, they can cause bodily injuries due to the existence of metallic objects contained in the landfills. The injuries might pave way for the entry of pathogens to cause other complications. As a result, they should be eliminated completely in order to ensure safety and good health.
Works Cited
Ambedkar, Shilaja N. AIDS in India. Jaipur, India: ABD Publishers, 2008. Print.
Eswarappa, Veda, and Sujata K. Bhatia. Naturally based biomaterials and therapeutics the case of India. New York, NY: Springer, 2013. Print.
Khoumbati, Khalil. Handbook of research on advances in health informatics and electronic healthcare applications global adoption and impact of information communication technologies. Hershey PA: Medical Information Science Reference, 2010. Print.
Sarkar, Atanu, and Srikanta K. Panigrahi. Vector-borne diseases in India: environmental health & policy perspectives. New Delhi: Manak Publications, 2007. Print.
Singh, Mohen Y. Emerging infectious diseases in India. New York: Nova Biomedical Books, 2009. Print.
Sorajjakool, Siroj, Mark F. Carr, and Julius J. Nam. World religions for healthcare professionals. New York: Routledge, 2010. Print.
Swaminathan, Jayashankar M.. Indian economic superpower fiction or future?. Singapore: World Scientific Pub., 2009. Print.
Thapa, Komilla, G. M. van der Aalsvoort, and Janak Pandey. Perspectives on learning disabilities in India current practices and prospects. Thousand Oaks: Sage Publications, 2008. Print.