Abstract
Ebola is one of the most severe viruses in the world. It was discovered in the Democratic Republic of Congo in 1976 and has continued to spread worldwide. The virus has caused several outbreaks in Africa, including Sierra Leone and DRC. Scientists are working on extensive research to learn more about the virus and develop the necessary treatments. This paper discusses the Ebola virus disease, including its transmission mode, symptoms, and prevention mechanism deeply. The genome makeup of the virus has also been discussed in the paper and the mechanism of replication in the body of the infected. The incubation period of the virus has been discussed and the major symptoms that the infected experience. The paper includes a visual representation of the virus and its infection rate.
Introduction
Ebola Virus Disease (EVD) is a severe viral illness transmitted through direct body contact with the infected person or animals. The Ebola virus originated in the Democratic Republic of Congo in 1976 and has caused several outbreaks (Rojas et al., 2). It is considered a zoonotic infection that can be transferred from an animal to a human being (Jacob et al., 25). The main form of transmission of the virus is through direct contact with the body fluids of the infected animal or person.
The first transmission is animal-to-human transmission, where the virus spreads to people through having a direct contract with the host animal’s blood and other body fluids. The second transmission is human-to-human transmission, where the infected person can spread the virus to other people (Berge 52). Furthermore, victims who have died of the Ebola virus can transmit it to those who have direct contact with the infected body. Scientists have also established animal-to-human transmission where the infected reservoir animal, considered a bat, can transmit the virus to other animals such as monkeys and antelopes (World Health Organization). Besides, if the infected person touches items, they become contaminated with the virus and can be transmitted to other people who touch them.
Disease Manifestation
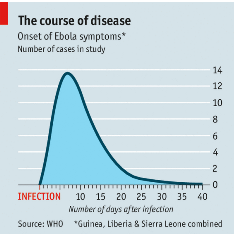
The Ebola virus manifests itself through various signs and symptoms. The infected person experiences symptoms within the first 2 to 21 days after infection. However, the average incubation period is 4 to 10 days (Yadav et al. 33). The Ebola symptoms have stages depending on the time of the infection. During the initial days of the infection, the infected people tend to show dry symptoms, which then progress to wet symptoms as the condition becomes severe. The dry symptoms include fatigue and pains, while the wet symptoms include vomiting and diarrhea. The primary symptoms of the Ebola virus have been closely associated with the symptoms of other infections such as malaria, influenza, and typhoid (Yadav et al. 36). These symptoms include fever, weakness and fatigue, sore throat, loss of appetite, severe headache and muscle pain, abdominal pains, and severe hemorrhaging and bleeding. Many victims have also shown signs of red eyes, hiccups, and skin rashes at the final stages of the disease.
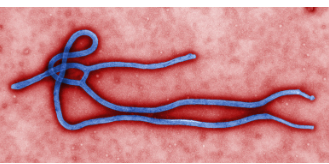
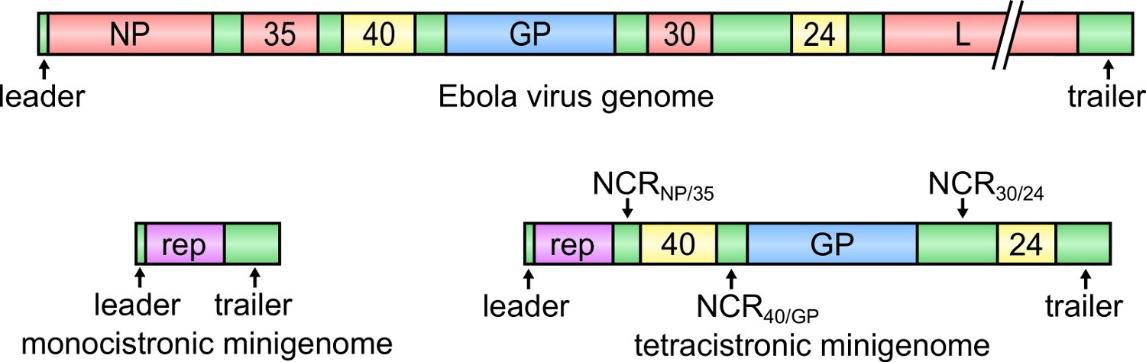
In humans, the Ebola Virus disease is caused by four major viruses of the Ebola Virus genus. They include the Sudan virus (SUDV), Bundibugyo virus (BDBV), the Ebola virus (EBOV), previously known as Zaire Ebola Virus, and the Tai Forest virus (TAFV) (Shu et al.). The ebolavirus is single-stranded and contains RNA genomes. The virus appears to be filamentous, with most of them being coiled or branched. They usually attack themselves at the surface of the cells of the receptors, then fuse with the affected cells by enveloping their cell membranes.
The virus significantly reduces the white blood cells’ ability to clot. Therefore, victims bleed in most openings, including the eyes, mouth, rectum, nose, or ears (Richards et al. 350). This condition is caused by internal leakage of the blood from smaller blood vessels. Leakage of blood may cause bleeding into the skin leading to various conditions, including purpura and hematomas (Richards et al. 352). Additionally, the blood may be present in the infected person’s stool and vomit.
Diagnosis
There is still research on the diagnostic methods that can be applied to confirm Ebola cases. However, the major laboratory indicators for detection include fluctuations in the number of white blood cells. The Ebola virus causes an imbalance in white blood cells where the cell count drops initially and then increases significantly. Furthermore, scientists rely on various liver enzymes, including aspartate aminotransferase (AST) and alanine aminotransferase (ALT) (Dixit et al. 15). The presence of the Ebola virus tends to increase the levels of these enzymes in the body of the infected person. Physicians can detect any abnormalities in the blood clotting, including prolonged bleeding time and unusual thromboplastin and prothrombin time.
The shape of the virus plays a significant role in the diagnosis process. Physicians observe the virus through the electron microscope to identify its unique filamentous forms (Brandt et al. 25). Furthermore, the virus can be diagnosed by detecting its RNA in the victim’s blood or by detecting antibodies formed against the virus in the infected person’s blood. This is the most reliable diagnostic method during the advanced stages of the infection. For the initial stages, scientists mostly rely on detecting the presence of proteins from the ELISA enzyme.
Treatment
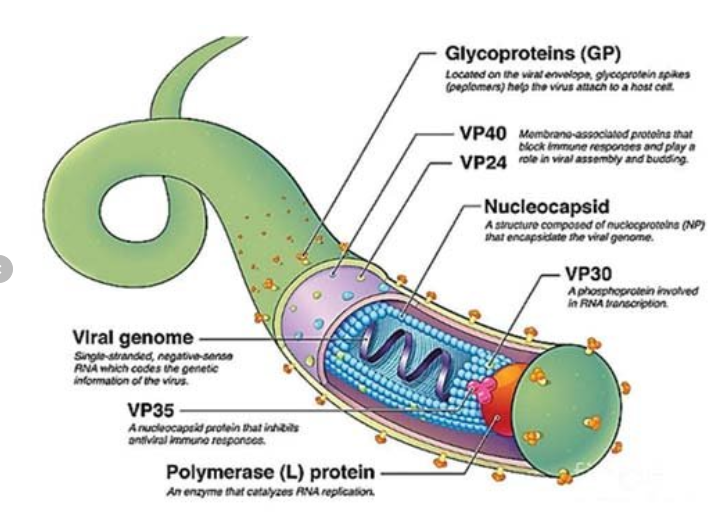
There is no universally approved treatment for the treatment of Ebola. However, the US Food and Drug Administration (FDA) approved two treatments that proved effective in treating the Zaire ebolavirus responsible for most outbreaks. The drugs include Inmazeb, approved in October 2020, and Ebanga drug, approved in December 2020 (Mulangu et al.). Inmazeb was developed by combining three monoclonal antibodies, while Ebanga contains one monoclonal antibody. The monoclonal antibodies are lab proteins manufactured to prevent the virus from replicating in the infected person’s body (Levine). The antibodies fight the Ebola virus by binding on the glycoprotein of the virus’s surface, limiting its ability to fuse with human cells.
Another method of handling the virus is subjecting the patient to supportive care. Various support care interventions for Ebola virus patients significantly increase their survival rate. They include providing the patients with body fluids through rehydration salts orally to enable the patients to recover lost body fluids. Moreover, the patient may be treated for symptoms such as nausea, fever, and various pains in the body, including muscle and joint pains. The pain is mostly relieved by administering painkillers certified by the World Health Organization (WHO). Some painkillers, such as aspirin and ibuprofen, may not be ideal for the treatment of Ebola because they are likely to cause further bleeding.
Prevention
Prevention has been deemed the best mechanism to prevent the spread of the Ebola virus. The first preventive mechanism is the administration of vaccines. In December 2019, the United States approved the first Ebola vaccine, rVSV-ZEBOV, which effectively protected people from getting infected ten days after taking the vaccine (Tomori and Kolawole 30). Caregivers have also been advised to wear protective clothing when handling the patients to minimize body contact, resulting in transmission. The protective gear for the Ebola caregivers includes gloves, masks, gowns, and goggles, which should leave no skin exposed. All the materials and items that the patients have come into contact with should be disinfected to prevent transmission of the virus to people who have contact with the infected objects (Hasan et al.). Some of the recommended disinfectants include detergents, and sodium hypochlorite, exposing the surfaces to temperatures above 60 degrees Celsius.
The World Health Organization (WHO) recommends regular washing of hands with soap and running water to prevent getting into contact with the virus. WHO advises people to maintain distance from the infected people to reduce the risk of having body contact that can result in an infection. Additionally, people should ensure that bush meat is appropriately handled using protective clothing. The meat should then be cooked thoroughly to ensure that all the germs and viruses present in the meat are killed.
Isolation and quarantine are highly recommended measures that easily prevent the spread of the virus. Isolation involves separating people who already have the virus from the general population that is not infected. Quarantine involves isolating people who may have been exposed to the virus but have not shown the symptoms. These mechanisms are essential to prevent an outbreak of the virus, whose transmission mode makes it highly contagious. Contact tracing has been a highly recommended mechanism to monitor the spread of the virus within the population and take early precautions to prevent an outbreak.
Pictures and Figures Representation
Conclusion
In conclusion, the Ebola virus spreads through direct body contact, making it highly contagious. The virus can be transmitted from human to human, animal to human, and animal to animal. The average incubation period for the virus is 4 to 10 days before the infected person starts to experience the symptoms. The major symptoms include fever, pain in the joints, diarrhea, vomiting, bleeding, and skin rashes. There is no globally certified treatment for the Ebola virus disease, but the use of monoclonal antibodies has proved effective. The best way to handle the virus is prevention which includes taking of vaccine and avoiding body contact with the infected person. It is recommended to wear protective clothing when attending to the infected person.
Works Cited
Berge, Tsanou, et al. “Modeling Ebola Virus Disease Transmissions with Reservoir in a Complex Virus Life Ecology.” Mathematical Biosciences & Engineering vol. 15, no. 1, 2018, p. 21.
Brandt, Janine, Lisa Wendt, and Thomas Hoenen. “Structure and Functions of The Ebola Virus Matrix Protein VP40.” Future Virology vol. 14, no. 1, 2019, pp. 21-30.
CDC. The Ebola Virus. 2022, Web.
Dixit, Devika, et al. “Review Of Ebola Virus Disease in Children–How Far Have We Come?.” Pediatrics and International Child Health vol. 41, no. 1, 2021, pp. 12-27.
DSI. Ebola Rate of Infection. 2022, Web.
Hasan, Shamimul, et al. “Ebola Virus: A Global Public Health Menace: A Narrative Review.” Journal of Family Medicine and Primary Care vol. 8, no. 7, 2019, p. 2189.
Jacob, Shevin T., et al. “Ebola Virus Disease.” Nature Reviews Disease Primers, vol. 6, no. 1, 2020, pp. 1-31.
JOVE. Ebola Virus Genome. 2022, Web.
Levine, Myron M. “Monoclonal Antibody Therapy for Ebola Virus Disease.” New England Journal of Medicine vol. 381, no.24, 2019, pp. 2365-2366.
Mulangu, Sabue, et al. “A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics.” New England Journal of Medicine vol. 381, 2019, pp. 2293-2303.
Richards, Guy A., Tim Baker, and Pravin Amin. “Ebola Virus Disease: Report from The Task Force on Tropical Diseases by The World Federation of Societies of Intensive and Critical Care Medicine.” Journal of Critical Care vol. 43, 2018, pp. 352-355.
Rojas, Manuel, et al. “Ebola Virus Disease: An Emerging and Re-Emerging Viral Threat.” Journal of Autoimmunity, vol. 106, 2020, p. 102375.
Shu, Qingbo, et al. “Species-Specific Quantification of circulating Ebolavirus Burden using VP40-Derived Peptide Variants.” PLoS Pathogens vol. 17, no. 11, 2021, pp. e1010039.
Tomori, Oyewale, and Matthew Olatunji Kolawole. “Ebola Virus Disease: Current Vaccine Solutions.” Current Opinion in Immunology vol. 71, 2021, pp. 27-33.
Viralzone. Ebola Filamentous Shape. 2022, Web.
World Health Organization. “Ebola Virus Disease Democratic Republic of Congo: External Situation Report 56.” Regional Office for Africa, 2019.
Yadav, Akshay R., and Shrinivas K. Mohite. “An Overview on Ebola Virus Disease.” Research Journal of Pharmaceutical Dosage Forms and Technology vol. 12, no. 4, 2020, pp. 267-270.