Childhood obesity is one of the most alarming health issues the US society is facing. Wright et al. (2016) state that approximately 30% of American children are overweight or obese. It has been acknowledged that obesity in children persists in their later life (Manios et al., 2013). This health condition is associated with the development of such serious disorders as diabetes mellitus, cardiovascular diseases, depression, and so on. Healthcare professionals utilize various strategies to address the issue.
The use of electronic health records (EHR) is regarded as one of the effective ways to treat obesity in this population (Cochran & Baus, 2015). The researchers claim that the use of EHR can be instrumental in diagnosing and developing treatment plans. These systems also help avoid medical errors. This paper includes a brief analysis of an effective EHR database that can be used when treating childhood obesity.
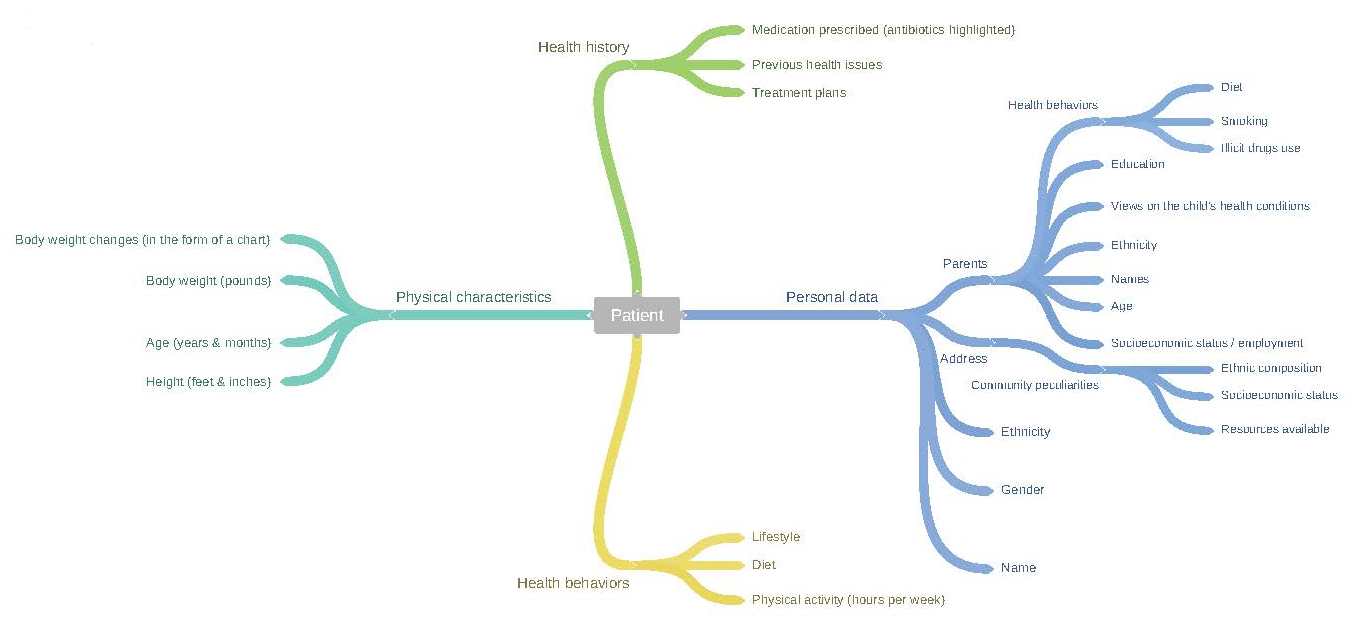
This database should include some basic personal data including the name, age, address, and so on. Such details are quite common for the existing databases. However, it is essential to expand the scope of the information by introducing such entities as community details. Address details cannot be enough as healthcare professionals are often unaware of the peculiarities of all communities while demographic data can help in understanding patients’ health conditions.
It is widely known that socioeconomic factors have a considerable effect on people’s health in general and childhood obesity in particular (Knai & McKee, 2010). Patients’ cultural peculiarities and socioeconomic status affect the ways healthy diets are seen and maintained. For instance, some populations (for example, Hispanic Americans) believe that there should be no restrictions regarding food, so body weight gain is regarded as something positive. Some communities can be characterized by the prevalence of the Latino or African American groups, which can shed light on these people’s health behaviors. Therefore, it is necessary to add such entities as ethnic peculiarities of the community, socioeconomic status, and the like. It is also necessary to include some data concerning the resources available in the community.
Furthermore, such details as gender, exact age, body weight, height, and so on are also quite common for EHR databases. The height should be noted in feet and inches. This precision is essential for the estimation of body weight gain. Patients’ weight can be measured in pounds. These measurements are widely used in the USA, and the vast majority of healthcare professionals understand them. As far as possible improvements in the existing EHR, body weight gain can also be traced in some systems, but it can be poorly presented (Manios et al., 2013).
It can be beneficial to develop an EHR system where body weight gain can be presented in the form of a chart. Healthcare professionals can note a patient’s body weight during every check-up while the system will create the chart that will help estimate the progress or increasing risks. This information should be provided in body mass index (BMI). Data concerning patients’ physical activity should also be one of the entities. The most appropriate measurement is hours per week. Such qualitative data as the information regarding patients’ lifestyle should also be present. Healthcare professionals can provide brief notes on the matter. Hobbies and interests can be noted.
An effective data management system should also include some data concerning patients’ previous treatment. The use of EHR is helpful as healthcare professionals can note and trace the use of different types of medication. When it comes to treating childhood obesity, it has been acknowledged that the use of antibiotics at early stages of life is associated with increased body weight gain in childhood (Bailey et al., 2014). Therefore, it can be important to develop an operation that highlights the use of antibiotics throughout patients’ health history. Healthcare professionals should be able to see the exact periods or dates when antibiotics were prescribed. Therefore, healthcare practitioners should pay specific attention to such records.
Some EHR systems include quite basic information about patients’ parents. Nevertheless, parental peculiarities, as well as their views, play an important role in the development of their children’s health behaviors and health conditions (Wright et al., 2016). For example, Wright et al. (2016) note that parents tend to underestimate the effects of their children’s body weight on their future health. Parents do not regard their children as obese or overweight although they believe that excessive weight can be associated with some health issues. As has been mentioned above, cultural peculiarities and ethnicity are important variables.
Therefore, the possible EHR system should include the corresponding entities. Such data as parents’ ethnicity, views on their children’s weight, their opinions concerning obesity and so on should be noted. Manios et al. (2013) stress that such information as maternal education and health behaviors (especially smoking) should be included as these factors are influential predictors of childhood obesity.
Finally, it is necessary to add that the data mentioned above should be presented in a drop-down menu. As many details as possible should be given in this form as it will help healthcare professionals to enter data quickly. Such data as gender, age, weight, body weight gain, lifestyle, diet, and other details can be presented in drop-down menus. Moreover, such qualitative data as parental options can be provided in this form. IT specialists can use the categories mentioned in other studies.
The CORE measurement developed by Manios et al. (2013) can be applied. The use of drop-down menus is also associated with fewer medical errors. The development of such systems will require the use of the existing data and certain research. It is essential to collect demographic data related to local communities. However, it is also vital to include space for notes and qualitative data. For example, Wright et al. (2016) explore parental views on their children health conditions, and the categories used by the researchers can be utilized. The proposed database will include several categories as shown below.
In conclusion, it is possible to note that an effective EHR database will include quantitative and qualitative data revealing the peculiarities of patients and their parents. Such details as gender, age, body weight, ethnicity, height, parental education, health habits, and opinion should be included. The system should have a drop-down menu that will help reduce the time needed to complete the database and decrease the number of medical errors. Some entities will still be given in the form of brief notes. The development of the new database will require the collaboration between healthcare professionals and IT specialists. The EHR system will also need secondary research aimed at revealing the existing health trends and cultural peculiarities of people living in the community.
References
Bailey, L., Forrest, C., Zhang, P., Richards, T., Livshits, A., & DeRusso, P. (2014). Association of antibiotics in infancy with early childhood obesity. JAMA Pediatrics, 168(11), 1063-1069.
Cochran, J., & Baus, A. (2015). Developing interventions for overweight and obese children using electronic health records data. Online Journal of Nursing Informatics, 19(1). Web.
Knai, C., & McKee, M. (2010). Tackling childhood obesity: The importance of understanding the context. Journal of Public Health, 32(4), 506-511.
Manios, Y., Birbilis, M., Moschonis, G., Birbilis, G., Mougios, V., Lionis, C., & Chrousos, G. (2013). Childhood obesity risk evaluation based on perinatal factors and family sociodemographic characteristics: CORE index. European Journal of Pediatrics, 172(4), 551-555.
Wright, D., Lozano, P., Dawson-Hahn, E., Christakis, D., Haaland, W., & Basu, A. (2016). Parental predictions and perceptions regarding long-term childhood obesity-related health risks. Academic Pediatrics, 16(5), 475-481.